

Cannabis News
What the DEA Gets Wrong about the Current Fentanyl Crisis

No, it’s not the Sinaloa Cartel – it’s Prohibition!
https://twitter.com/CarlitoS_lim/status/1694124572759527465?s=20
The DEA is once again missing the forest for the trees in its assessment that the sons of “El Chapo” are primarily responsible for scaling up fentanyl production and trafficking after their father’s arrest. While they may be significant players, the DEA fails to acknowledge how their own policies created the conditions that allowed fentanyl to become such a scourge.
The DEA acts as if drug cartels operate in a vacuum, when nothing could be further from the truth. Cartels like Sinaloa exist because of prohibition. For over 50 years, the US has waged a War on Drugs that has completely failed to reduce drug supply or demand. Instead, it has artificially inflated the profits of illicit drugs by pushing the drug trade into the hands of criminal organizations. With no legal market competition, groups like Sinaloa can charge astronomical prices.
The demand for opioids, both legal and illegal, has proven extremely inelastic. When the DEA restricts the prescription opioid supply, which they have done aggressively since the early 2010s, desperate people turn to the black market. With the legal supply diminished, criminal organizations rush to fill the void.
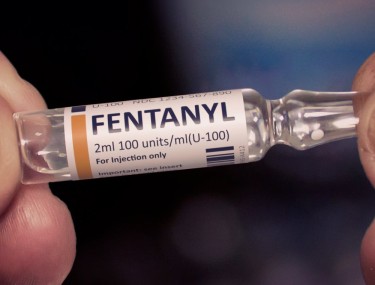
Fentanyl offers cartels an ideal product. It’s synthetic, so it doesn’t rely on the supply of plant-based drugs like heroin. It’s also incredibly potent, allowing traffickers to smuggle small amounts across the border. One kilogram of fentanyl contains 500,000 doses and is worth over $1 million on the street. The profits are staggering compared to the minimal production costs.
Yet fentanyl is also far more dangerous than traditional opioids. Even tiny dosing errors can be fatal. Illicit fentanyl has become a leading driver of the overdose crisis, with over 60,000 deaths in 2020 alone. But just as with El Chapo’s marijuana and cocaine trade, the fault lies first and foremost with prohibition.
The DEA also fails to consider its own complicity in El Chapo’s rise to power. For decades, the DEA worked closely with Mexican authorities in the War on Drugs. This partnership was frequently corrupted by individuals on both sides of the border profiting from the drug war and even directly enabling trafficking. The incentive for corruption under prohibition is simply too high.
El Chapo rose in power not just despite the DEA’s efforts, but in many ways because of them. And now the same cycle continues with his sons and associates like El Mayo. These black market dynamics will persist as long as the DEA tries vainly to prohibit human nature and market economics.
The tragic irony at the heart of the opioid crisis is that stricter prohibition led to stronger drugs. Similarly, defeating El Chapo led to more fentanyl. The DEA needs to fundamentally rethink its role. Only by moving to harm reduction over endless drug warring can we ameliorate this ongoing American tragedy.
How do you combat Fentanyl? You legalize heroin of course!
The fentanyl crisis devastating America will not end through prohibition and policing. The only solution that can effectively undermine the black market poisoning our communities with fentanyl is full legalization and harm reduction, starting with legal heroin.
Many balk at the idea of legal heroin, but it would be far safer than the current unregulated market flooded with fentanyl. When people overdose on street drugs, it’s usually because potency is unpredictable. Legal heroin with consistent dosing removes this risk. Further, providing pharmaceutical-grade heroin for free through supervised injection sites would completely decimate the cartels’ customer base.
Free heroin programs have been implemented successfully in several countries. Switzerland pioneered the approach in the 1990s, giving prescription heroin to addicts who failed other treatments. Over two decades, the program has slashed drug-related deaths, stabalized addicts’ lives, and decriminalized addiction.
Portugal enacted a similar policy, becoming the first country to fully decriminalize all drug possession in 2001. Again, the results confounded critics. Overdose deaths and HIV infections dropped significantly, and the number of people in treatment doubled. By taking a health approach instead of criminal justice, Portugal improved public safety and welfare.
The data is clear that addressing the opioid crisis with treatment and harm reduction works better than prohibition, criminalization, and stigmatization. Unfortunately, the DEA and much of America’s law enforcement infrastructure remain committed to the failed War on Drugs.
But we know from history that prohibition does not end problematic substance use—it just empowers criminals and underground markets. Alcohol prohibition gave rise to Al Capone, modern drug prohibition El Chapo. Only by legalizing substances can we regulate them for safety and undermine criminal profiteering.
Fentanyl has infiltrated the drug supply because it maximizes smuggling profits. But few would seek it out if provided legal, regulated alternatives like heroin. It may seem counterintuitive, but giving away heroin is the only way to combat fentanyl.
Rather than wasting billions on DEA budgets every year, we could run free heroin programs. If the goal is saving lives and improving public health, the solution is apparent. Any deaths under a legal heroin program would be tragic but still fewer than the tens of thousands dying from fentanyl annually.
The opioid crisis requires America to shed its ideological commitment to prohibition. Our choice is not between saving lives with prohibition or abandoning drug users to addiction. Proven harm reduction approaches can restore dignity and stabilize people’s lives. Ending the War on Drugs is the only path to finally defeating the damage of cartels and lacing of drugs like fentanyl. The sooner we accept this, the more lives will be saved.
Why forcing addicts to quit drugs is counterproductive and dangerous!
Trying to force addicts into recovery before they are ready is not just futile, but dangerous. Research shows that rehab and abstinence programs have poor success rates when participation is coerced rather than voluntary.
According to studies, only about 2-5% of people pressured into rehab by courts or families achieve long-term sobriety. Most quickly relapse when the external pressure is removed. This is because imposed rehab does not address the underlying reasons why people use drugs. Healing cannot be compelled.
Trying to make addicts quit before they choose to leads to dangerous cycles of relapse and self-medication. Criminalizing addiction makes suffering worse by removing stable life foundations like housing, families, and work.
A better approach is stabilizing addicts’ lives with compassion, not judgment. Providing safe housing, clean paraphernalia, addiction medications like methadone, and health resources reduces harm. Building a sense of community and belonging addresses addiction’s roots in trauma, isolation, and despair.
With caring support, addicted persons can progressively reduce their drug use and transition to abstinence. But this must be their own choice. Forced rehab merely engenders distrust and resistance. Meeting drug users where they are at and giving them autonomy over recovery has the best outcomes.
The War on Drugs tries to impose sobriety through prohibition and punishment. But addiction is a disease, not a moral failure. We must move from condemnation to open arms, from control to empowerment. Only then can we end the overdose crisis ravaging our communities. For addicted lives matter too.
It’s time to nullify the Controlled Substance Act and renegotiate Drug Policies!
The fentanyl crisis has underscored the abject failure of America’s War on Drugs. Each year, the human toll of overdoses and mass incarceration grows, while cartel violence terrorizes our southern border. We pursue this failed policy based on a false dichotomy – that our only options are either the current prohibitionist approach or totally abandoning drug users to addiction. In reality, the solution lies in a third path – harm reduction and decriminalization.
To enact this sensible reform, we must nullify the Controlled Substances Act that serves as the legal bedrock of prohibition. This Nixon-era law categorizes drugs into schedules largely based on moral judgements rather than pharmacological facts. It arbitrarily separates “legal” and “illegal” substances without scientific rationale. This ideological law does not curb drug use – it just empowers black markets and criminal organizations.
In effect, the Controlled Substances Act created a government-enforced monopoly for the pharmaceutical industry to peddle its own addictive drugs. Big Pharma helped spawn the opioid crisis through deceptive and irresponsible marketing of oxycontin and vicodin. It lobbies to keep plant-based competitors like cannabis and psychedelics prohibited. The DEA acts as its enforcement arm, violently suppressing any threats to this pharmaceutically-driven drug monopoly.
It is time to acknowledge that cognitive liberty and the authority over one’s consciousness is a basic human right. While certain substances like alcohol and heroin carry risks, experience shows prohibition does far more harm than drug use itself. Education, harm reduction, and voluntary treatment provide a more ethical and effective approach.
Decriminalizing possession would keep nonviolent users out of prison. Legalizing natural psychoactive plants could help many mental health conditions. Providing pharmaceutical-grade opioids in safe injection sites would halt fentanyl overdoses. We know these measures work because they have succeeded in countries like Switzerland, Portugal, and Canada.
America’s drug policies do not have to be dominated by ignorance, racism, and moral panic. We can base them on science, liberty, and compassion instead. But this begins with grassroots advocacy. Every voter should demand their representatives support drug policy reform. Local ballot initiatives are powerful tools as well.
The younger generations do not buy into “reefer madness” propaganda; they know the Drug War has been an abysmal failure. The politicians still carrying water for these harmful policies are relics of the past. Their day is done. The future lies in ending the racist, unethical, disastrous Controlled Substances Act regime. Only when we reclaim autonomy over our minds and bodies can we meaningfully address the overdose crisis. It starts by legalizing freedom.
FENTANYL AND WEED, READ ON…









Edible Arrangements Leans into Intoxicating Hemp Products: A Strategic Expansion
Edible Arrangements, a brand renowned for its vibrant fruit bouquets and sweet treats, is embarking on a bold new venture into the hemp and THC-infused edibles market. Through its parent company, Edible Brands, the company has launched Edibles.com, an e-commerce platform offering a variety of hemp-based products such as THC-infused beverages, gummies, and snacks. This strategic move taps into the burgeoning demand for cannabis-related wellness products and reflects a deliberate expansion beyond traditional offerings.
Introduction to Edible Arrangements and Its New Venture
Edible Arrangements was founded in 1999 by Tariq Farid, who envisioned a unique way to gift fresh fruit arrangements that were both visually appealing and delicious. Over the years, the company has grown to become a global brand with hundreds of locations across the United States and internationally. However, the company’s latest initiative marks a significant departure from its traditional fruit-based offerings, signaling a broader strategic shift towards becoming a comprehensive food, health, and wellness company.
The New Venture: Edibles.com
Edibles.com debuted on March 20, 2025, starting operations in Texas with ambitious plans to expand rapidly across Southeastern states like Florida and Georgia. The platform is designed to cater to consumers aged 21 and older, providing low-dose THC products that comply with the 2018 Farm Bill, which legalized hemp containing less than 0.3% THC by dry weight. Select products will also be available for nationwide shipping where legally permitted, leveraging the company’s existing logistics infrastructure.
Product Lineup
The initial product lineup includes a range of THC-infused beverages, gummies, and snacks. These products are designed to appeal to both seasoned cannabis users and newcomers looking for low-dose, accessible options. The company emphasizes the importance of quality and safety, ensuring that all products undergo rigorous testing to meet high standards of purity and potency.
Strategic Alignment and Market Potential
The move into the infused edibles market aligns with Edible Brands’ vision of becoming a broader food, health, and wellness company. CEO Somia Farid Silber highlighted that the infused edibles market is a fast-growing sector with high consumer demand for safe and reliable products. The company is leveraging its extensive franchise network to deliver these items while planning to open brick-and-mortar stores under the Incredible Edibles brand.
Market Trends and Consumer Demand
The cannabis industry, particularly the segment focused on hemp and THC-infused products, has seen exponential growth in recent years. This growth is driven by increasing consumer interest in wellness and recreational products, as well as evolving legal landscapes that have opened up new markets. Edible Arrangements is positioning itself to capitalize on this trend by offering products that cater to both health-conscious consumers and those seeking unique gifting options.
Challenges and Opportunities
While this expansion offers significant growth potential, it also comes with challenges such as navigating varying state regulations and ensuring product safety and quality. The company aims to address these issues through robust infrastructure and consumer advocacy. Thomas Winstanley, a cannabis industry veteran leading Edibles.com, emphasized the company’s unique position to drive innovation in this emerging market.
Regulatory Challenges
One of the primary challenges facing Edible Arrangements is the complex regulatory environment surrounding cannabis products. Laws regarding the sale and distribution of THC-infused products vary significantly from state to state, requiring the company to adapt its operations to comply with local regulations. This includes ensuring that products meet specific THC content limits and are marketed responsibly.
Quality Control and Safety
Another critical challenge is maintaining high standards of quality and safety across all products. Edible Arrangements is investing heavily in testing and quality assurance processes to ensure that all products meet stringent safety standards. This includes partnering with reputable suppliers and implementing rigorous testing protocols to verify the potency and purity of all THC-infused items.
Consumer Education and Advocacy
As part of its strategy, Edible Arrangements is also focusing on consumer education and advocacy. The company recognizes that many consumers are new to cannabis products and may have questions about usage, dosage, and safety. To address this, Edibles.com will provide comprehensive product information, dosage guidelines, and resources for consumers to learn more about the benefits and risks associated with THC-infused products.
Marketing Strategy
Edible Arrangements plans to leverage its existing brand recognition and customer loyalty to promote its new line of hemp-based products. The company will utilize social media, email marketing, and targeted advertising to reach its target audience. Additionally, partnerships with influencers and cannabis industry experts will help build credibility and drive awareness about the brand’s entry into this new market.
Future Expansion Plans
In the coming months, Edible Arrangements plans to expand its operations beyond Texas, targeting key markets in the Southeast. The company is also exploring opportunities to open physical stores under the Incredible Edibles brand, which will offer a curated selection of THC-infused products alongside traditional Edible Arrangements items.
Incredible Edibles Stores
The Incredible Edibles stores will serve as a unique retail experience, combining the company’s traditional fruit arrangements with its new line of hemp-based products. This format will allow customers to explore and purchase THC-infused items in a welcoming and educational environment. The stores will also host workshops and events focused on cannabis education and wellness, further enhancing the brand’s position as a leader in this emerging market.
Conclusion
Edible Arrangements’ foray into the hemp and THC-infused edibles market marks a significant strategic shift for the company. By leveraging its brand recognition and logistical capabilities, Edible Arrangements is poised to become a major player in this rapidly growing sector. While challenges exist, the company’s commitment to quality, safety, and consumer education positions it well for success in this new venture.
As the cannabis industry continues to evolve, Edible Arrangements’ entry into this market underscores the broader trend of mainstream brands embracing cannabis-related products. This move not only expands the company’s offerings but also reflects a broader cultural shift towards greater acceptance and normalization of cannabis use.
HEMP-DERIVED THC DELIVERIES ARE HERE, READ ON…



California Supreme Court Upholds Cannabis Legalization
In a landmark decision, the California Supreme Court recently reaffirmed the legality of cannabis in the state by de-publishing a prior appellate ruling. This move effectively prevents the lower court’s opinion from being used as legal precedent in future cases, ensuring that California’s cannabis laws remain intact. The decision is a significant victory for the state’s legal cannabis industry and reinforces California’s position as a leader in cannabis legalization.
Background of the Case
The case, JCCrandall v. County of Santa Barbara, originated from a lawsuit filed by Lompoc property owner Janna Caron Crandall. She challenged the County of Santa Barbara’s decision to allow cannabis transportation on an easement road crossing her property. Crandall argued that the easement’s terms prohibited federally illegal activities, thus making the county’s permit approval unlawful. This challenge was rooted in the fact that cannabis remains illegal under federal law, despite being legalized in California.
The Legal Framework
California legalized recreational cannabis in 2016 with the passage of Proposition 64, also known as the Adult Use of Marijuana Act (AUMA). This law allowed adults 21 years and older to possess and use cannabis for recreational purposes. However, the federal government still classifies cannabis as a Schedule I controlled substance, making it illegal under federal law. This dichotomy between state and federal laws has created legal complexities and challenges for cannabis businesses operating in California.
The Appellate Court Ruling
In January 2025, the Court of Appeal sided with Crandall, suggesting that California’s cannabis regulations were unlawful due to cannabis being federally illegal. This ruling was seen as a potential threat to the state’s cannabis industry, as it implied that federal law could preempt state laws allowing cannabis use and sale. The appellate court’s decision was based on the argument that the easement agreement prohibited activities that were illegal under federal law, and since cannabis is federally illegal, allowing its transportation on the easement would violate the terms of the agreement.
Implications of the Appellate Ruling
If the appellate court’s decision had stood, it could have had far-reaching implications for California’s cannabis industry. It would have potentially opened the door for similar challenges to cannabis operations across the state, undermining the legal framework that has been established since Proposition 64. This could have led to increased legal uncertainty and risk for cannabis businesses, potentially stifling growth and investment in the sector.
The Supreme Court Decision
The California Supreme Court’s decision to de-publish the appellate court’s ruling effectively nullifies its impact as a legal precedent. This means that the opinion cannot be cited or relied upon in future cases, ensuring that California’s cannabis laws remain secure. The Supreme Court’s action was in response to a request from the Department of Cannabis Control and other stakeholders who sought to protect the state’s cannabis regulations.
Statement from the Department of Cannabis Control
“We are pleased that the Court agreed to address that Court of Appeal decision at the Department of Cannabis Control’s request, supporting California law and its legal cannabis industry,” said DCC Director Nicole Elliott. This statement reflects the relief and support within the industry and regulatory bodies for the Supreme Court’s decision.
Impact of the Supreme Court Decision
The Supreme Court’s decision has several key implications for California’s cannabis industry and the broader legal landscape:
-
Legal Certainty: By preventing the appellate court’s opinion from being used as precedent, the Supreme Court has provided legal certainty for cannabis businesses. This clarity is crucial for investors, operators, and consumers alike, as it ensures that the industry can continue to operate without the threat of federal preemption being used to undermine state laws.
-
Industry Growth: The decision supports the continued growth and development of California’s cannabis industry. With legal certainty, businesses are more likely to invest in expansion, innovation, and compliance, which can lead to increased economic benefits for the state.
-
Regulatory Framework: The ruling reinforces the authority of state regulatory bodies, such as the Department of Cannabis Control, to oversee and enforce cannabis laws. This ensures that the industry operates within a well-defined legal framework, which is essential for maintaining public safety and trust.
-
Consumer Access: For consumers, the decision means that access to legal cannabis will remain unchanged. This is important for both recreational users and patients who rely on cannabis for medical purposes.
-
Federal-State Relations: While the decision does not change federal law, it underscores the ongoing tension between state and federal cannabis policies. It highlights the need for continued advocacy for federal reform to align with the growing number of states that have legalized cannabis.
Historical Context of Cannabis Legalization in California
California has been at the forefront of cannabis legalization efforts in the United States. The state’s journey towards legalizing cannabis began with the passage of Proposition 215 in 1996, which allowed for the medical use of cannabis. This was followed by Proposition 64 in 2016, which legalized recreational cannabis.
Proposition 215: Compassionate Use Act
Proposition 215, also known as the Compassionate Use Act, was a groundbreaking piece of legislation that allowed patients with certain medical conditions to use cannabis with a doctor’s recommendation. This law marked the beginning of a shift in public perception and legal treatment of cannabis, paving the way for broader legalization efforts.
Proposition 64: Adult Use of Marijuana Act (AUMA)
Proposition 64 expanded on Proposition 215 by legalizing the recreational use of cannabis for adults. It established a regulatory framework for the cultivation, distribution, and sale of cannabis, creating a multibillion-dollar industry in California. The law also included provisions for taxation, licensing, and environmental protection.
Challenges and Opportunities in the Cannabis Industry
Despite the legal victories, the cannabis industry in California faces several challenges:
-
Regulatory Compliance: Businesses must navigate complex state and local regulations, which can be costly and time-consuming. Compliance with these regulations is essential to avoid legal issues and maintain operational licenses.
-
Market Competition: The California cannabis market is highly competitive, with many licensed operators competing for market share. This competition can drive innovation but also poses challenges for smaller businesses trying to establish themselves.
-
Federal Banking Restrictions: Due to federal illegality, cannabis businesses often face difficulties accessing traditional banking services. This forces many companies to operate largely in cash, which can increase security risks and complicate financial management.
-
Environmental Concerns: Cannabis cultivation can have environmental impacts, such as water usage and energy consumption. The industry Is working to address these concerns through sustainable practices and regulatory compliance.
-
Social Equity Programs: California has implemented social equity programs aimed at supporting individuals and communities disproportionately affected by the war on drugs. These programs provide resources and opportunities for entry into the cannabis industry.
Future of Cannabis Legalization
The California Supreme Court’s decision is part of a broader national conversation about cannabis legalization. As more states legalize cannabis, there is growing pressure for federal reform. Several bills have been introduced in Congress to address issues such as banking access and federal preemption, but comprehensive reform remains elusive.
Federal Reform Efforts
Efforts to reform federal cannabis laws include bills like the MORE Act, which would decriminalize cannabis at the federal level, and the SAFE Banking Act, which aims to provide banking access to cannabis businesses. While these bills have seen progress, they face significant hurdles in becoming law.
International Perspectives
Internationally, countries like Canada and Uruguay have fully legalized cannabis, providing models for how federal legalization could work. These countries have established national regulatory frameworks that address issues like taxation, public health, and international trade.
Conclusion
The California Supreme Court’s decision to uphold the legality of cannabis in the state is a significant victory for the industry and its stakeholders. It ensures that California can continue to lead in cannabis legalization and regulation, providing a model for other states and countries. As the legal landscape evolves, it is crucial for ongoing advocacy and reform efforts to address the remaining challenges and opportunities in the cannabis sector.
CANNABIS IN CALIFORNIA HAS PROBLEMS, READ ON…



Cannabis daily can help people get off opioids (STUDY)
As Donald Trump continues to trudge on in his second term, he’s made it abundantly clear that tackling the fentanyl crisis is high on his agenda. The rhetoric is bold and aggressive – promises to go after cartels with military force, threats against drug dealers, and a generally hawkish stance toward drug trafficking. It’s the kind of tough talk that plays well to his base, but the question remains: will it actually solve anything?
If we look at his appointments and policy directions, it seems we’re heading for War on Drugs 2.0 rather than an innovative approach to a complex problem. History has taught us that you can’t simply bomb, arrest, or threaten your way out of drug epidemics. These tactics have been tried for decades with little success.
There is, however, one solution hiding in plain sight that could revolutionize Trump’s approach to the opioid crisis – cannabis legalization. Yes, you read that correctly. If Trump were to take the bold step of federally legalizing cannabis, he could potentially cement his legacy as one of the most transformative presidents in modern history.
It sounds counterintuitive at first – fighting drugs with another drug? But the evidence is mounting that cannabis could be a powerful weapon against opioid addiction and overdose deaths. Recent studies are showing promising connections between cannabis use and reduced opioid dependency.
So how exactly would legalizing a plant help combat the deadliest drug crisis in American history? Well, let me tell you!
A groundbreaking study published last week in the journal Drug and Alcohol Review has added significant weight to the argument that cannabis could help combat the opioid crisis. The research, conducted by an eight-person team from the British Columbia Centre on Substance Abuse, the University of British Columbia, and Simon Fraser University, examined data from 1,242 people who used drugs while also living with chronic pain.
Their findings were striking: “Participants reporting daily cannabis use exhibited higher rates of cessation compared to less frequent users or non-users.” In other words, those who used cannabis every day were more likely to quit using opioids altogether. This effect was particularly pronounced among men, suggesting “potential differences in cannabis use behavior and effects” between sexes.
This isn’t an isolated finding. A growing body of research supports the idea that cannabis can serve as an effective substitute for opioids. A federally funded study found that in states with legal marijuana, prescriptions for opioid pain medications dropped significantly among commercially insured adults. Another study discovered that legalizing medical cannabis appeared to significantly reduce payments from opioid manufacturers to doctors specializing in pain management – further evidence that cannabis was replacing prescription painkillers.
Perhaps most compelling is the research linking cannabis legalization to reduced fatal opioid overdoses. One study estimated that recreational marijuana legalization “is associated with a decrease of approximately 3.5 deaths per 100,000 individuals.” When you consider that over 107,000 Americans died from drug overdoses in 2021 alone (with 75% involving opioids), the potential life-saving impact becomes clear.
The opioid crisis has ravaged communities across America, destroying families and costing the economy an estimated $1.5 trillion annually in healthcare costs, criminal justice expenses, and lost productivity. Cannabis legalization offers a multi-pronged solution: it provides a safer alternative for pain management, reduces dependency on opioids, and potentially saves thousands of lives each year.
Beyond addressing the opioid epidemic, legalizing cannabis would create hundreds of thousands of new jobs, generate billions in tax revenue, reduce unnecessary incarcerations (particularly in communities of color), and open up new avenues for medical research and international commerce.
For a businessman-turned-president like Trump, the economic case alone should be compelling. The question is whether he has the vision to seize this opportunity or if he’s too beholden to interests that benefit from prohibition – pharmaceutical companies, private prisons, and law enforcement agencies that rely on drug war funding. If he truly wants a slam dunk policy that would address the fentanyl crisis while creating jobs and stimulating the economy, cannabis legalization could be his legacy-defining move.
While we wait for politicians to catch up with science, those suffering from chronic pain or other conditions treatable with cannabis might consider a more immediate solution: growing your own medicine.
Now, let me be crystal clear – I’m not advocating breaking the law. If cannabis is illegal in your state, I don’t want you risking arrest and criminal charges. However, speaking personally, if I were suffering from chronic pain and had few options, I might consider a small, discreet grow operation of 2-4 plants. This would be my absolute secret – something I’d never discuss with anyone, ever.
The beauty of growing your own cannabis extends far beyond just having a supply of medicine. There’s something profoundly therapeutic about nurturing a plant from seed to harvest. You develop patience, attention to detail, and a deeper connection to the plant medicine you’re creating. It’s a relationship, not just a transaction.
When you grow your own cannabis, you also know exactly what’s in it. No pesticides, no mysterious contaminants – just pure plant medicine cultivated with care. You can select strains specifically bred for your conditions, whether that’s pain, anxiety, insomnia, or inflammation. The process puts the power of healing back in your hands.
Beyond the primary flower, home growers can make use of every part of the plant. Fan leaves can be juiced for their non-psychoactive cannabinoid content. Trim can be used to make topicals or edibles. Even the stems can be used to make teas or tinctures. Nothing goes to waste.
There’s also a significant cost advantage. A small home grow can produce enough medicine to last months, potentially saving thousands of dollars compared to dispensary prices. For those on fixed incomes or without insurance coverage for their conditions, this economic benefit can’t be overstated.
I firmly believe that any meaningful cannabis legalization bill must include provisions for home cultivation. Without the right to grow your own medicine, legalization is merely transferring authority from one controlling entity to another. It’s still authoritarianism masquerading as freedom, just with different gatekeepers.
The right to grow is fundamental to true cannabis freedom. It acknowledges the plant for what it is – a natural resource that should be accessible to all, not just those who can afford to purchase it from state-sanctioned vendors. Home cultivation empowers individuals to take control of their own health without excessive dependence on either the black market or corporate cannabis.
While we push for policy change at the federal level, let’s not forget that sometimes the most revolutionary act is simply planting a seed.
The evidence is overwhelming: we’re facing an unprecedented opioid epidemic that’s claiming thousands of American lives every year, and cannabis represents a viable, evidence-based solution to this crisis. The latest research confirming that daily cannabis use can help people quit opioids adds to the mountain of data supporting cannabis as a harm reduction tool.
Yet despite the scientific consensus, I’m not holding my breath for federal action. The sad reality is that most politicians on both sides of the aisle receive substantial funding from industries that benefit directly from cannabis prohibition – pharmaceutical companies pushing their own patented pain medications, private prison corporations dependent on drug offenders to fill beds, and police departments that receive military-grade equipment through drug war budgets.
These entrenched interests have billions of reasons to maintain the status quo, and they’ve proven remarkably effective at delaying meaningful reform for decades. Even as public opinion has shifted dramatically in favor of legalization, with roughly two-thirds of Americans now supporting it, policy changes creep along at a glacial pace.
Perhaps Trump, with his penchant for disruption and unpredictability, could surprise us all by embracing cannabis reform as part of his anti-fentanyl strategy. It would certainly align with his populist messaging and “America First” economic policies. A thriving legal cannabis industry would create jobs, boost tax revenues, and potentially save countless lives from opioid overdoses.
I can hope for such bold leadership, but I’ll continue preparing for the long, slow grind of incremental progress. In the meantime, the opioid crisis rages on, claiming lives that could potentially be saved with a plant that’s been used medicinally for thousands of years. If that’s not a tragedy of policy failure, I don’t know what is.
CANNABIS TO REDUCE OPIOID USE, READ ON…
DR. OZ SAYS CANNABIS CAN GET PEOPLE OFF OPIOIDS, HOW DOES IT WORK?

Getting THC Edibles in Your Edible Arrangement?

Is Cannabis Legal in California Right Now?

Germany: Trial against operator of Trier cannabis vending machine discontinued

The best energizing THC gummies of 2025 by Leafly

Mixed Messages From The Feds About Cannabis

Humboldt County extends deadline to pay marijuana cultivation taxes

How Hemp Helps You Sleep

420 in Texas is at Reggie & Dro

Daily Cannabis Use Can Help People Get Off Opioids (STUDY)

The Future of Cannabis and Sleep Medicine

Distressed Cannabis Business Takeaways – Canna Law Blog™

United States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)

What you Need to Know

Drug Testing for Marijuana – The Joint Blog

NCIA Write About Their Equity Scholarship Program

It has been a wild news week – here’s how CBD and weed can help you relax

Cannabis, alcohol firm SNDL loses CA$372.4 million in 2022

A new April 20 cannabis contest includes a $40,000 purse

Your Go-To Source for Cannabis Logos and Designs

UArizona launches online cannabis compliance online course
-
 Cannabis News2 years ago
Cannabis News2 years agoDistressed Cannabis Business Takeaways – Canna Law Blog™
-
 One-Hit Wonders2 years ago
One-Hit Wonders2 years agoUnited States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)
-
 Cannabis 1012 years ago
Cannabis 1012 years agoWhat you Need to Know
-
 drug testing1 year ago
drug testing1 year agoDrug Testing for Marijuana – The Joint Blog
-
 Education2 years ago
Education2 years agoNCIA Write About Their Equity Scholarship Program
-
 Cannabis2 years ago
Cannabis2 years agoIt has been a wild news week – here’s how CBD and weed can help you relax
-
 Marijuana Business Daily2 years ago
Marijuana Business Daily2 years agoCannabis, alcohol firm SNDL loses CA$372.4 million in 2022
-
 California2 years ago
California2 years agoA new April 20 cannabis contest includes a $40,000 purse