

Psychedelics
ABC News Australia: Australia is about to legalise MDMA and psilocybin for medicinal use. So how will it work?

Psychedelics
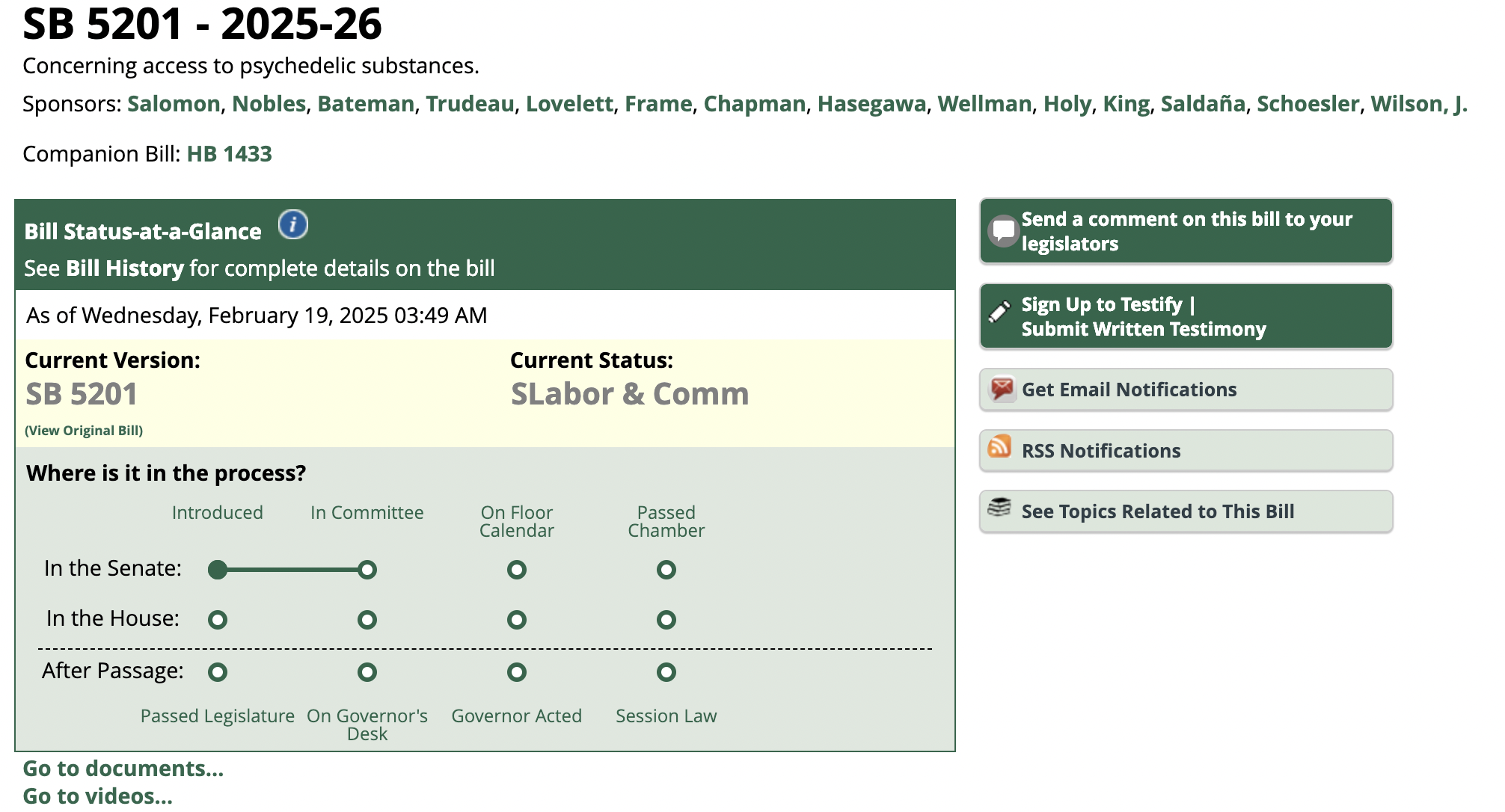
Linked In Post – Jon Dennis, Psychedelic Lawyer: Washington SB 5201, the regulated psilocybin access bill, was considered today by the Senate Committee on Labor & Commerce ( 18 Feb 2025)

Washington SB 5201, the regulated psilocybin access bill, was considered today by the Senate Committee on Labor & Commerce. The bill would require low-income and other taxpayers to subsidize regulated access that is cost-prohibitive for many, while continuing to criminalize the same activities outside of the regulated marketplace.
For context, Oregon’s regulated system was promised to be self-funded by licensing fees and sales taxes, but the program needed a $3.1MM bailout in 2023, and the program is now seeking an additional $3.5MM bailout from the legislature. This is despite already-exorbitant licensing fees, including a $2,000 annual fee for facilitators. (By contrast, the annual fee for an Oregon law license is $683; the annual fee for medical doctors is $702.)

Taxing residents for the administration of a costly access program, while criminalizing affordable access outside the program, is problematic–particularly in Washington where local governments representing 14% of the entire population have already called on state lawmakers to decriminalize psilocybin and other plant-based psychedelic substances. Washington lawmakers must do better and not ignore the socio-economic and criminal justice impacts of a regulated-only access program.
Psychedelics
Alert: We are just over a week away from the Natural Medicine Division opening our application process to individuals who are interested in becoming business Owners or Natural Medicine Handlers, and to business applications for Healing Centers, Cultivations, Testing Facilities and Product Manufacturers.
An actress in Mexico tragically lost her life after she ingested Amazonian frog venom as a part of a cleansing ritual while at a spiritual retreat. She experienced severe diarrhoea after taking part in the ceremony and was rushed to a hospital, but the doctors failed to save her life.

The 33-year-old actress Marcela Alcázar Rodríguez took part in the traditional South American Kambo ritual, which involves drinking water, getting burns on the body, and ingesting frog venom to cleanse the body of toxins, reported the Mirror. However, this ritual is known to have deadly consequences.
How is the Kambo ritual performed?
The participants in the ritual are made to drink more than a litre of water. Small burns are then created on their skin, following which frog mucus is applied on the wounds.

The mucus, which contains venom, increases blood pressure and induces vomiting, reported the outlet. It also causes diarrhoea in some cases. Other symptoms involve fainting, dizziness, swollen lips and face. Usually, the symptoms last for nearly half an hour. However, extended exposure of the venom to the blood stream can cause seizures and also death.
What happened to Marcela Alcázar Rodríguez?
Soon after beginning the ritual, Rodríguez reportedly started throwing up and eventually suffered from severe diarrhoea – these symptoms are often considered the body’s “healing” reactions during the cleansing process. Initially, she refused help but gave in when her friend visited her.
According to the Metro, a shaman at the retreat in Mayocoyani, Durango, told her she couldn’t leave. However, after her condition worsened, the person fled. Reportedly, police are now searching for the shaman.
Tribute to the actress
In a social media post, Durango Film Guild paid tribute to the actress after her untimely demise. They remembered her as “a young woman who worked in various short films, series and movies filmed in Durango.”
The guild added, “She leaves a void in the hearts of the people who knew her working in what she loved: cinema.”

Minnesota: Ishkode cannabis dispensary is now open at Vermilion

Ohio House Republicans’ cannabis measure a ‘slap in face,’ NORML says

Save 30% all month long at The Dispensary Fulton

Ohioans activate to defend weed legalization from lawmakers

It All Turned A Bit Bogan At Aussie Medical Cannabis Symposium

Building cannabis brands that reach across markets

ILGM’s Home Grow Tour 2025

Should Medical Marijuana Be Allowed in Worker’s Comp Claims?
Karma Koala Podcast 238: Daniel Shortt Launches New Firm With Partner Perry Salzhauer In Pacific NW
Trump invites former cannabis prisoner to speech, but doesn’t mention cannabis (Newsletter: February 5, 2025)

Distressed Cannabis Business Takeaways – Canna Law Blog™

United States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)

What you Need to Know

Drug Testing for Marijuana – The Joint Blog

NCIA Write About Their Equity Scholarship Program

It has been a wild news week – here’s how CBD and weed can help you relax

Cannabis, alcohol firm SNDL loses CA$372.4 million in 2022

A new April 20 cannabis contest includes a $40,000 purse

Your Go-To Source for Cannabis Logos and Designs

UArizona launches online cannabis compliance online course
-
 Cannabis News2 years ago
Cannabis News2 years agoDistressed Cannabis Business Takeaways – Canna Law Blog™
-
 One-Hit Wonders2 years ago
One-Hit Wonders2 years agoUnited States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)
-
 Cannabis 1012 years ago
Cannabis 1012 years agoWhat you Need to Know
-
 drug testing1 year ago
drug testing1 year agoDrug Testing for Marijuana – The Joint Blog
-
 Education2 years ago
Education2 years agoNCIA Write About Their Equity Scholarship Program
-
 Cannabis2 years ago
Cannabis2 years agoIt has been a wild news week – here’s how CBD and weed can help you relax
-
 Marijuana Business Daily2 years ago
Marijuana Business Daily2 years agoCannabis, alcohol firm SNDL loses CA$372.4 million in 2022
-
 California2 years ago
California2 years agoA new April 20 cannabis contest includes a $40,000 purse