

Cannabis News
Is a Meth Head a Criminal or a Patient?


When it comes to guilty pleasures – Twitter for me is a mix of bittersweet toxicity. While it’s true, there’s a lot of interesting takes and opinions by millions of interesting characters…it’s also a never-ending pit of people shouting at each other.
While this inherently isn’t a bad thing if you’re into getting into digital shout-offs, to me it’s a colossal waste of time.
As a writer, I try to find interesting angles, unique perspectives, and to keep my finger on the pulse of the collective chaos of humanity in order to write, create, ponder on things most people take for granted.
When it comes to cannabis, the War on Drugs, Prohibition, the history of drugs, etc – I’ve spent more than a decade of my life distilling information into articles which I published on multiple platforms. My pseudonym, “Reginal Reefer” has thousands of published articles – some of them serious, others absolute insanity.
However, even when I write about things that seem incredible, I always to keep an “anchor” in reality. My job is not to convince you whether something is or isn’t, but to merely spark the imagination on the “possibilities” associated with a concept.
I was mindlessly – yes, mindlessly – scrolling through Twitter and saw a tweet about global drug decriminalization, of which I responded, “We should rather enshrine the right to bodily autonomy as an inalienable human right”…or something along those lines.
Some people agreed.
Some didn’t.
This is a story about one who “didn’t” and instead of me engaging with the user on the platform, I decided to utilize a technique I use to stay creative.
You can call it a sort of “emotional alchemy” where you take a digital response from a stranger, and turn it into a greater work that provides more value to the world.
For example, some rando responds to my tweet and for some reason triggers an emotional response – instead of putting up my dukes and trying to outwit the twit, I rather take a few giant steps backwards and write about it…as I am doing right now.
This allows me to take the emotion – which is motivating me to take action, and reframe it in a more positive direction. One could also call it a kind of emotional Aikido.
This is what I intend to do.
Before continuing however, I’m not going to mention the name of the person nor his handle as this is not the point of the article.
I need his words, not his identity.
The reason I bring this up is because in one of our exchanges where I excused his opinion based on the anonymity of his account, saying, “If you don’t have the balls to stand by what you say…”
Of which he replied;
You think im gonna ID myself for some leftist that spews a narrative they clearly don’t fully grasp? Im sure you are well versed in the “natural” side of drug use, but clearly dont understand things like modern synthetics and their devastating impacts.
We’re already off to a good start. The nameless person assumed I have a political “side” where I lean towards. Little does he know I’m the one sitting on the side lines watching the two sides battle it out as their corporate masters bet on the winners.
However, instead of prolonging the debate, I wanted to address a specific point that the anonymous writer tweeted about, and I think it actually has some real value.
I’ll try to summarize the sentiment of Mr. Anonymous below;
So by your logic, needing Narcan (danger to themselves) one time is enough to intervene? Also, if they want to stay an addict, fine; but society doesnt have to fund for that lifestyle either.
What was my logic?
Unless the “addict” is breaking a law and posing a danger to themselves or others – the addict should be allowed to be addicted and should be provided means of escaping the addiction if he or she decides to do so.
Coffee Drinkers are addicts but we don’t jail them…
But why did I say this in the first place? It was actually a response to his comment;
Addicts do not make rational decisions. When drug use is so severe, someone else needs to make some decisions to interrupt the behavior.
And this is where we begin our exploration of the concept of giving addicts drugs for free.
However, I understand if you’re confused at this point, so let me summarize the sentiment of “Mr. Anonymous” to help establish the premise of our article;
Claim: Addicts do not make rational decisions and therefore if one is addicted severely then someone else needs to make the decision for you to interrupt your behavior.
Welcome to the Grey…
While the claim seems logical. If someone is suffering from severe addiction, someone else must override their autonomy and set them on the straight path.
Except, at what point does addiction become problematic? As I said earlier, “coffee addicts are severely addicted…” yet one wouldn’t consider that a “problematic addiction”.
If that’s the case, we need to create a distinction in addiction. “Socially accepted non-destructive addiction” and “socially abhorred destructive addiction”.
However, we already have rules for that. Meaning, if you break these laws, your addiction has “stepped out of bounds” of what is socially accepted and permitted. If you mug an old lady to buy drugs – you committed a crime of assault against another person.
However, the act of using drugs should not be considered a “crime” in that scenario. Because by designating “drug use” as a category of criminal behavior, it means that by default all addicts of illicit drugs are criminals.
Under this definition, the state can rightfully revoke their freedom and turn them into property of the state…which is what has been happening under the guise of “drug prohibition” for over fifty years.
So the first thing we have to understand in this debate is that we have a fundamental issue with drug prohibition that stands in direct contrast to human autonomy. Furthermore, the selective nature of drug prohibition also creates fundamental clashes with how prohibition is enforced.
Why is it that you don’t criminalize alcohol consumption, or to be more technical, “The consumption of ethanol”, which is a mind altering substance that not only claims lives due to excess consumption, is linked to 40% of all violent crimes according to the FBI data?
This drug gets a free pass. It’s not even on the Controlled Substance Act.
But why? Could it be that they tried to prohibit it in the past, realized that drug prohibition was a colossal failure that only reaped death, corruption, and violence? I wonder if that had any parallels to the sheer amount of carnage left in the wake of the War on Drugs?
When Mr. Anonymous said, “Last time I checked, coffee drinkers generally are not robbing and stealing to support their habit, staying up for weeks at a time, and swinging machetes around.”
When pointing out that using the term “addicts” would include coffee drinkers, he pointed out that coffee drinkers don’t engage in violent or detrimental behaviors. Which is true for the most part.
However, alcohol drinkers do. They get behind wheels of cars, they crash and kill people. They get drunk and violent. They rape, steal, and murder.
Therefore, under the logic of Mr. Anonymous – we should prohibit alcohol as it qualifies all of the metrics designated by him.
However, we know that this won’t happen.
Alcohol isn’t even regulated by the DEA. It got lumped with another agency regulating Alcohol, Tobacco and Fire Arms and Explosives. Why they are regulating alcohol, tobacco and fire arms as a singular category still baffles the mind – but this is how bureaucracy works.
Nonetheless, we can see a complete incongruence when it comes to how drug regulation works from a general policy perspective. There’s obvious special interests involved and this is by design.
The “Legal drugs” are controlled by Pharma.
The Illegal Drugs are all “suppressed” by the DEA.
For years, in conjunction with the FDA, NIDA and government sponsored propaganda – The war on Drugs effectively established a drug monopoly for Big Pharma.
Alcohol & Tobacco were given exception due to their influence within the government prior to the drafting of the 1971 Controlled Substance Act signed into law by Richard Nixon. The same Nixon that took the US off the Gold Standard and created the corporate Clusterfuck, which is our current reality.
But I digress.
To summarize my point here is that unless we have equity in drug enforcement or a unilateral application of policy on all drugs – then to prohibit “some people” because their particular drug create undesirable outcomes – that would literally be discrimination.
Now I’d like to point out – getting hooked on Meth – the drug Mr. Anonymous used as his reason for supporting his opinion.
I agree with him, that people hooked on meth and that are creating havoc due to their addiction would probably need some intervention, however, unless they are physically breaking laws other than consuming a drug – then we should technically leave them to their own devices.
This – for better or worse – is the fundamental principle of bodily autonomy. You have a right to your own body – meaning, you can fuck it up all the way to your own death. Will some people fuck it up? Most certainly – but this is a fundamental right to individual liberty that if we give the power to the government – you cease to have that right.
If saying “this drug” gives me a right to remove your personal liberty because of “these reasons”, yet those same reasons apply to other accepted drugs – your argument fails to have substance due to the hypocrisy of enforcement.
Therefore, unless you are absolutely on board with banning alcohol in the same capacity as other “dangerous drugs” – you’re not actually upset about the negative consequences of drug use, but rather the negative outcomes of certain drugs and its impact on society.
Why giving Meth to a Meth head could be the best way to deal with a Meth head…
Here’s a question. When is a meth head most dangerous?
The answer is, “When they don’t have drugs and no means of getting more!”
When their addiction becomes overwhelming, they typically turn to theft and on occasions, assault. Once they buy their drugs, they return to the sweet faux-comfort of their perpetual misery. Their temporary alleviation from their turmoil.
One way to address this situation is to force a junkie into reforming their life. You can arrest them, send them to a drug court, mandate rehab that has to either be funded privately or publically, and hope it sticks.
However, the evidence isn’t really in favor of this working. As this Healthline Article outlines;
A 2016 report by the Massachusetts Department of Public Health found that people who were involuntarily committed were more than twice as likely to die of an opioid-related overdose than those who chose to go into treatment.
Another 2016 study published in the International Journal of Drug Policy found little evidence that mandatory drug treatment helps people stop using drugs or reduces criminal recidivism.
“There appears to be as much evidence that [compulsory treatment] is ineffective, or in fact harmful, as there is evidence that it is effective,” said study author Dan Werb, PhD, who’s also an epidemiologist and policy analyst at the University of California at San Diego (UCSD).
Most of the studies reviewed by Werb and his colleagues looked at involuntary drug treatment centers outside the United States, many of which are rife with human rights violations.
“What we’ve seen across the world — in Mexico and Southeast Asia and China — is that ‘treatment centers’ that are mandated can effectively turn into internment camps,” Werb said.
A 2018 study done in Tijuana, Mexico, by Claudia Rafful, a doctoral student in public health at UCSD, found that involuntary drug treatment is also associated with an increased risk of nonfatal drug overdoses.
Part of this may be due to loss of tolerance to the drugs when someone suddenly stops using them. This happens not just with mandatory treatment, but also when people end up in jail.
Across the board, forcing people into rehab isn’t showing much effectiveness.
In fact, it seems that it could be doing the opposite, increasing fatal overdoses and not reforming anyone.
These forced rehab clinics are often funded by taxpayers, meaning that even though they are paying for it – they aren’t getting the returns they are seeking.
So if straight up drug prohibition doesn’t work, and forced rehabilitation doesn’t work – what options do we have?
Give them the drugs for free!
In an ideal world, everyone would be able to engage with anything and hold themselves accountable. Unfortunately, this is the real world and some people will develop habits that aren’t “up to par” with the rest of society.
They will get addicted and some of them will turn to theft or violence when they are faced with the “hunger” of addiction.
But the real question is, “When does the junkie’s drug use become a problem for society?”
The answer is, “when the junkie turns to criminal behavior to sustain their habit”.
If a junkie were to steal or mug people for resources, this would create a chain reaction. First of all, the perceived safety of the given area begins to diminish as the odds of getting robbed or mugged increases.
This in turn increases police activity, which has a social cost as we’re paying wages with our taxes. The policing will inevitably lead to arrest which then activates the whole legal system economy. Court appointed lawyers, paperwork, food, water, etc…all of the extra things will be paid by the taxpayer.
At the end of the day, maintaining the current system “costs” a lot of money to society with very little benefit.
The taxpayer is paying for the treatment, the police activity, etc – and the junkie doesn’t recover.
Conversely, producing heroin cheaply if legalized would be very possible. Not to mention, you’d have control over purity – same for meth. You’d be able to provide the meth head with a similar addiction, but cleaner – for free.
This would remove the incentive of the junkie to resort to criminal behavior. Why rob someone, face potential jail time, have a record – when you can walk to a center, which will give you drugs for free.
Some might think this as a crazy idea, however – it’s one of the only ideas that have real world effectiveness.
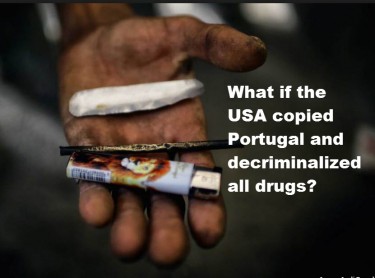
In places like Portugal and Switzerland, they have programs where all drugs are decriminalized, and centers of drug consumption. In Switzerland, they have a center where people can consume heroin.
The addict walks into the front door, asks for a dose – after filing some paperwork and signing liability forms, they are escorted to a comfortable room, where they are handed as much drugs as they want without inducing a fatal dose – and then they trip.
When they are ready to walk out of the front door – they can.
Nobody is forcing them to go to rehab, no one is forcing them to stop doing drugs. All they are doing is removing the hazardous elements of severe drug addiction.
They are removing the incentive to rob or turn to violence. They are removing the element of bad hygiene in terms of sharing needles and so forth. They created a controlled space where hardcore addicts can trip, and simultaneously reduced the “harm and violence” associated with severe drug use.
The results?
They saw a drop in crime, disease, violence, across the board. The same happened in Portugal when they stopped treating drugs as a “thing to be stopped” as opposed to “helping people cope”.
The average age of a junkie rose to over 30, meaning that younger people weren’t as motivated to consume drugs under this model. Perhaps, it’s because you remove the incentive for the black market to compete with a “free market”.
Perhaps it’s because socially, drug addiction is seen as a health problem, and thus – the youth distances themselves from use…who knows.
What we do know is that it’s providing more positive results than negative ones. More importantly, it treats addicts as humans, it gives them the option to quite, but also makes it safer for the consumer and society as a whole.
Sure, not every country is the same and potentially you’d need to create specific demographical conditions – but it seems to me that after 50+ years of prohibition and decades of forced rehabilitation – perhaps it’s time we change strategies.
Perhaps it’s time we rethink drugs altogether, remove the monopoly that Pharma has on drug production and distribution. Maybe we take science and rework the framework on how we interpret “problematic drug use”, and create policies that actually benefit society.
Why should we pay the junkie their drugs? Because it reduces the overall burden on society in terms of violence, crime and economy.
Drug use is here to stay…
The truth of the matter is that there will always be a portion of the population that will consume drugs and get severely addicted. They aren’t bad people. They typically come from broken, fatherless homes – they have little perceived support and have little self control.
But it’s important to understand that this is a small portion of drug users. This isn’t the norm. The vast majority of drug users, whether they consume cannabis, psychedelics, or other drugs – do not develop an addiction.
The vast majority of drug users, save highly addictive ones (that I argue we should give for free), they can consume and leave it without a problem.
Yet, we decided to punish everyone for the faults of a few. If this is the case, then we should also ban fast food for the obese, since this is the number one killer in their demographic and they too are addicted. They too cost the taxpayer billions annually…but if we go down that road – can we call ourselves a free society?
Our job is not to control other people’s behavior, but empower them to make better choices. We do this by accepting their condition, by providing safer alternatives, and saying, “If you want out of the addiction cycle – you can walk this way and we can help you…but it’s your choice!
I believe this is the only way to deal with dangerous drug addiction, while reducing the influence of the black market on drugs in general.
More importantly, removing the Drug War mechanisms that have only served as a cancer on society is of paramount importance if we ever want to achieve a state of actual liberty. We need to recognize that people will use drugs, and that is their choice…and that’s okay as long as they aren’t hurting others.
And that’s what I believe after 15 years of writing on these topics…
DECRIMINALIZE ALL DRUGS, READ ON…








The Rise and Fall of the Cannabis Industry
The cannabis industry has undergone a radical transformation over the past forty years. What began as an obscure and illegal activity hidden in the shadows has blossomed into a multi-billion dollar industry that spans across multiple states and even countries. However, this evolution hasn’t come without significant growing pains. Is Trump 2.0 part of a new avenue for cannabis?
Throughout this journey, we’ve witnessed both tremendous benefits and troubling issues emerge from a complex web of factors: overregulation that strangles small businesses, persistent black market competition that undercuts legal operators, and federal government interference that creates a patchwork of contradictory policies.
Today, we’re going to explore a region that could be considered the birthplace of American cannabis culture – Humboldt County and the broader Emerald Triangle of Northern California. This legendary growing region helped put cannabis on the map long before dispensaries dotted urban landscapes and corporate cannabis became a reality.
Let’s dive into how this iconic marijuana mecca rose to prominence, flourished during the golden years, and now faces an uncertain future as the industry continues to evolve beneath the weight of legalization’s complicated aftermath.
Let’s go!
Though I’ve never personally visited Humboldt County, its reputation in cannabis culture is legendary. Those winding roads through towering redwoods and misty mountains have become almost mythical in the stories told by those who’ve made the pilgrimage to America’s most famous growing region.
The cannabis industry in Humboldt didn’t spring up overnight. It has roots stretching back to the counterculture movement of the 1960s, when idealistic young people fled urban centers in search of simpler, more authentic lives. These back-to-the-landers discovered that the region’s remote location and ideal growing conditions made it perfect for cultivating cannabis—a crop that could actually sustain their pursuit of alternative lifestyles.
What began as a means of self-sufficiency for hippie communes soon evolved into something much more substantial. According to Paul Modic’s historical account of Humboldt’s cannabis industry, the price per pound jumped from $1,000 in 1975 to a staggering $5,000 by the early ’90s. With these kinds of returns, cannabis cultivation in the Emerald Triangle transformed from a countercultural statement into a serious economic engine.
Modic refers to this economic boon as “the Green Nipple,” a colorful term suggesting how the industry nourished an entire regional economy. Growers were able to build homes, raise families, support local businesses, and create a unique culture that blended environmental consciousness with a fiercely independent spirit. During these boom years, cannabis money flowed freely through communities like Garberville, Redway, and Willits, supporting everything from hardware stores to schools.
But as with any gold rush, the good times couldn’t last forever. The passage of Proposition 215 in 1996, which legalized medical marijuana in California, marked the beginning of significant change. While seemingly a victory for cannabis advocates, it inadvertently opened the floodgates for increased production. As more people jumped into cultivation, supply increased and prices began their long, steady decline.
By the early 2010s, according to Modic, the “Green Nipple” had transformed into what he aptly calls the “Green Monkey”—were you riding it, or was it riding you? Growers had to dramatically scale up operations just to maintain their previous income levels. Where once a modest garden could support a family, now multiple light-deprivation greenhouses and larger grows became necessary.
The stress of managing larger operations brought new challenges: more workers to supervise, increased risk of crop failure from pests or mold, and the perennial challenge of finding buyers for ever-larger harvests. As Modic points out, these stresses replaced the previous concerns about “cops and helicopters,” which had “mostly disappeared from the list of stresses by then.”
Little did these growers know that the real challenges were still to come, as full legalization loomed on the horizon and would forever change the landscape they had helped create.
On November 8, 2016, California voters passed Proposition 64, legalizing recreational cannabis use throughout the state. For decades, legalization had been the rallying cry for cannabis activists, the holy grail that would end prohibition and usher in a new era of freedom and prosperity. But for many small farmers in Humboldt County, legalization would prove to be a poisoned chalice.
The promise of legalization was seductive: no more helicopter raids, no more fear of prison, and legitimate business status. What wasn’t as apparent was the bureaucratic nightmare awaiting those who chose to enter the legal market.
Modic’s account provides several telling examples of farmers who attempted to navigate the new legal landscape, only to find themselves drowning in expenses and red tape. He writes about “one grower from Salmon Creek” who went to the bank and reported, “Estelle told me it would cost $20,000 to go legal, now I’ve got $100,000 into it and it’s a big hassle, but I’m in too deep to stop and have to keep trying to finish the paperwork.”
Another farmer from Ettersburg, according to Modic, was “complaining that it had already cost him a few hundred thousand dollars to ‘come into compliance,’ he was still far from getting his license, and if he could do it all over, he wouldn’t.” Modic later observed that this once “handsome and youthful-looking” farmer was later spotted “looking old and haggard, and still struggling with his large weed farm.”
The regulatory requirements for legal operation proved to be prohibitively complex and expensive. Environmental impact reports, water rights documentation, building permits for structures that had existed for decades, application fees, consultancy costs—the list went on and on.
The California Department of Fish and Wildlife became a particular obstacle for many farmers. Modic tells the story of “a former clone dealer from Sprowel Creek” who had a property with a spring that “started and stopped on his forty acres, one of the state requirements for licensing.” Despite this seemingly perfect setup, when Fish and Wildlife examined his land, they “discovered damage from logging decades before he bought it back in the seventies, and the expensive remediation costs would be more than the land was worth.” The farmer had no choice but to dump the property “at a loss.”
Meanwhile, as small farmers struggled to navigate the regulatory labyrinth, large corporations with significant financial backing moved in. These operations could afford compliance costs and were positioned to produce cannabis at scale, driving prices even lower. The pound price, which had already fallen to around $1,000 post-medical legalization, plummeted to $500 and then to a devastating $250 after recreational legalization, according to Modic’s account.
For context, when prices were $5,000 per pound, a farmer could make a good living with just 20 pounds per year. At $250 per pound, that same farmer would need to produce 400 pounds just to maintain their income—a scale impossible for many small operations and certainly not feasible within the constraints of legal permits for small grows.
The cruel irony wasn’t lost on the community: the very plant that had enabled generations to live independently in this rural paradise was now, under legalization, becoming the instrument of their economic demise. For many, the choice became stark: attempt to operate legally and face financial ruin, continue growing illicitly with increased risk, or abandon cannabis cultivation altogether.
As Modic notes, “businesses in town have closed, the hills have emptied out, and would-be farmers who got in late and have large land payments are abandoning their land.” The promise of legalization was revealing itself to be a complex and often devastating reality for the very communities that had built California’s cannabis industry.
When California voters approved recreational cannabis, many predicted the black market would quickly fade away. After all, why would consumers take risks with illegal purchases when they could simply walk into a licensed dispensary? Why would growers continue operating in the shadows when they could run legitimate businesses?
The reality has proven far more complicated, and the black market hasn’t just survived—in many ways, it’s thrived.
Industry analysts estimate that in 2022, California’s legal cannabis market generated approximately $5.3 billion in sales—impressive until you consider that the state’s illicit market was estimated to be worth $8 billion or more. Despite legalization, the majority of cannabis consumption in California still occurs outside the regulated system.
For Humboldt farmers, the persistence of the black market presents both an opportunity and a dilemma. As Modic observes in his historical account, “Many of those who are able to stay are looking for regular jobs with which to survive in this depressed economy, as the pound price plummets to $250.” However, he also notes that “there’s still farmers with good connections growing and selling like it’s 2008, and may have a few good years left.”
This suggests a divided industry where those with established out-of-state connections can still find buyers willing to pay premium prices, especially in prohibition states where cannabis remains scarce. However, this path comes with significant risks. Federal enforcement remains a threat, especially for interstate trafficking. Furthermore, as more states legalize and develop their own cannabis industries, these out-of-state markets become increasingly competitive.
The more troubling aspect of the thriving black market is what it reveals about the legal framework California has created. When licensed businesses struggle to compete with illicit operations, it suggests fundamental flaws in the regulatory system. The excessive taxation—which can reach 40% when combining state excise tax, local taxes, and other fees—creates an insurmountable price gap between legal and illegal cannabis.
Additionally, the limited number of licensed retail outlets throughout the state means many consumers don’t have convenient access to legal cannabis. With approximately 75% of California municipalities banning cannabis businesses, vast “cannabis deserts” exist where consumers have no choice but to turn to the black market.
For Humboldt’s legal growers, this dynamic is particularly frustrating. They’ve invested heavily in compliance, only to watch their illicit competitors undercut them without consequence. Many legal operations resort to what industry insiders sometimes call “diversion”—selling a portion of their crop into the illicit market to remain financially viable.
This reality points to a broader failure in California’s approach to legalization. Rather than creating a functioning legal market that could absorb and transform existing cannabis operations, the state has inadvertently strengthened the very black market it sought to eliminate.
For Humboldt County, this means the cannabis economy continues to operate in a precarious gray zone—neither fully legal nor completely illicit, with participants forced to navigate an increasingly complex and risky landscape.
Perhaps the most important question raised by the transformation of Humboldt’s cannabis industry concerns the fate of the pioneers who built it. As Modic asks in his historical account, “What’s going to happen to all those back-to-the-landers and old growers, now in their seventies and eighties, still living in their off-grid cabins in the middle of nowhere, without the steady income they had over the last forty years, and no retirement plan?”
It’s a profound question that highlights the human cost of this industrial transformation. For decades, these growers operated outside traditional economic systems. They didn’t have 401(k)s or pensions. Their retirement plan was their land and their annual cannabis crop. Now, with prices at historic lows and their physical ability to manage farms diminishing with age, many face an uncertain future.
Some have managed to sell their properties to younger growers or to transplants seeking rural lifestyles, but the collapse in cannabis prices has significantly devalued land throughout the region. Properties that might have sold for millions during the boom years now struggle to find buyers at a fraction of those prices.
Others have attempted to transition to different crops or businesses, with varying degrees of success. There are nascent efforts to develop Humboldt as a cannabis tourism destination, leveraging the region’s storied reputation. Some farms have opened for tours, created farm-stay experiences, or developed educational programs about cannabis cultivation.
Local support networks have emerged as well. Community organizations provide assistance to aging growers, helping them access social services they might have avoided during their years operating in the illegal market. There are food banks specifically serving rural communities and mutual aid networks where neighbors help neighbors.
County and state officials have largely failed to address this looming crisis. The same regulators who created nearly impossible compliance requirements for small farmers have offered little in terms of support for those displaced by the industry’s transformation. There are no pension programs for retired cannabis farmers, no transitional assistance for those whose livelihoods have evaporated.
The situation represents a broader ethical question about legalization: what responsibility do we have to those who built an industry while it was still illegal? These pioneers took significant risks, faced potential imprisonment, and developed the cannabis varieties and cultivation techniques that the legal industry now profits from. Yet they’ve been largely abandoned in the rush toward corporate cannabis.
For communities throughout Humboldt County, the human cost of this transition is impossible to ignore. Empty storefronts in once-thriving towns, properties reclaimed by banks, and elderly residents struggling to survive are the visible manifestations of an economic collapse that could have been mitigated with more thoughtful regulation.
The pioneers of Humboldt’s cannabis industry didn’t just grow a plant—they created a culture and an economy that sustained thousands of people for generations. As that era comes to a close, we must confront difficult questions about what we owe to those who came before and how we might create a more inclusive cannabis industry moving forward.
After reviewing historical accounts like Modic’s and analyzing reports from throughout the region, I’ve come to a sobering conclusion: what we’re witnessing isn’t simply market evolution but rather a deliberate transfer of wealth and opportunity from small independent producers to large corporate interests.
The cannabis industry that sustained generations of Humboldt residents wasn’t perfect. It operated outside the law, sometimes attracted unsavory elements, and certainly had environmental impacts. But it also represented something uniquely American—a decentralized economy where individuals with limited capital could build sustainable livelihoods through their own labor and ingenuity.
The promise of legalization was that it would bring these operations into the light, providing consumer protection while allowing the existing industry to thrive legally. Instead, the regulatory framework that emerged seems almost perfectly designed to eliminate small producers while creating opportunities for well-capitalized newcomers.
This doesn’t appear to be accidental. The excessive regulatory requirements, the high cost of compliance, the limited retail licenses, and the heavy tax burden combine to create insurmountable barriers for small operators. Meanwhile, large multi-state operators can absorb these costs while scaling up production to maintain profitability despite falling prices.
For consumers, this transformation means less diversity in cannabis products, as corporate cultivation favors high-yield strains over the unique varieties developed by Humboldt’s craft growers. For communities, it means the loss of an economic engine that supported everything from schools to social services through the circulation of cannabis dollars.
Most troublingly, the current regulatory regime has failed to achieve even its stated goals. The black market remains robust, suggesting that the legal framework hasn’t created a functioning alternative. Environmental issues persist, both from non-compliant grows and from the massive legal operations that have replaced smaller farms.
Looking forward, there are potential paths to improvement. Reduced tax burdens could help legal operators compete with the black market. Streamlined regulations could make compliance achievable for small farmers. Interstate commerce, if eventually permitted, could open new markets for California’s producers. Craft cannabis designations, similar to wine appellations, could help small farmers distinguish their products in the marketplace.
But for many of Humboldt’s original cannabis families, these changes would come too late. The community and culture they built over decades is already unraveling, a casualty of well-intentioned but fundamentally flawed legalization policies.
The rise and fall of Humboldt’s cannabis industry serves as a cautionary tale for other regions pursuing legalization. It demonstrates that how we legalize matters just as much as whether we legalize. If we truly value diversity, sustainability, and opportunity in the cannabis space, we must create regulatory frameworks that support these values rather than undermining them.
For those of us who care about cannabis culture and the communities built around it, the challenge now is to advocate for policies that preserve what was valuable about the legacy market while addressing its legitimate problems. The alternative—a cannabis industry dominated by the same corporate interests that control so many other sectors of our economy—would represent a profound loss, not just for cannabis consumers but for American culture as a whole.
INSPIRATION:
kymkemp.com/2025/02/21/sohum-history-the-rise-and-fall-of-the-marijuana-industry/
https://kymkemp.com/2025/02/21/sohum-history-the-rise-and-fall-of-the-marijuana-industry/
TRUMP ON CANNABIS THE SECOND TIME AROUND, READ ON…

WHAT DOES TRUMP’S NEW CANNABIS POLICY LOOK LIKE?

Rethinking Marijuana Legalization: A Response to the National Review
Cannabis legalization has swept across America in waves, creating a patchwork of policies that vary dramatically from state to state. Some jurisdictions embrace full recreational use, others permit medical applications only, while some maintain total prohibition. This inconsistent legal landscape makes it nearly impossible to accurately measure the success or failure of legalization efforts. Without uniform policies and implementations, any cost-benefit analysis becomes murky at best.
In this fragmented environment, opinions about cannabis legalization remain sharply divided. Some celebrate newfound freedoms and opportunities, while others lament perceived social costs and unintended consequences. The National Review recently published an opinion piece questioning whether we should reconsider marijuana legalization altogether, citing several issues they believe undermine the case for legal cannabis.
Today, I’m going to examine these claims with a critical eye. While I agree that we absolutely should “rethink” marijuana legalization, my conclusion differs dramatically from the National Review’s perspective. Rather than retreating from legalization, I believe we need to push forward with more comprehensive reforms that address the legitimate concerns while delivering on the promised benefits.
The current half-measures and regulatory inconsistencies have created a situation where neither prohibitionists nor advocates are satisfied with the outcomes. Only through thoughtful, evidence-based policy adjustments can we realize the full potential of legalization while minimizing downsides. So yes, let’s rethink marijuana legalization – but let’s make sure we’re using all the available data and considering the root causes of any implementation problems.
The National Review piece relies heavily on arguments from Manhattan Institute Senior Fellow Steven Malanga, who suggests legalization has failed to deliver on its promises. The article highlights several key complaints:
-
The pervasive smell of marijuana in public spaces
-
Failure to eliminate black markets
-
Disappointing tax revenue that sometimes requires taxpayer subsidies
-
Increased usage rates contrary to predictions
-
Health concerns, particularly regarding psychosis
-
Perceived connections between cannabis and “social breakdown”
Let’s tackle these points one by one:
The Smell: While cannabis odor can be noticeable, this concern fundamentally misunderstands the concept of liberty in a diverse society. If someone is consuming cannabis in their private residence or in designated areas, their personal choices shouldn’t be criminalized simply because others find the smell unpleasant. Just as we accommodate cigarette smokers in designated areas and don’t ban cooking pungent foods, cannabis consumption can be managed through reasonable time, place, and manner restrictions. The development of cannabis social clubs, similar to cigar lounges, would further localize any odor concerns.
Black Markets:
The persistence of illicit markets isn’t a failure of legalization itself but rather of its incomplete implementation. Black markets thrive precisely because cannabis remains federally illegal, creating banking restrictions, interstate commerce prohibitions, and excessive regulatory burdens that drive up costs for legal operators. States with more reasonable tax structures and fewer arbitrary licensing caps have seen significantly less illicit market activity.
Tax Revenue:
Despite claims to the contrary, legal cannabis has generated billions in tax revenue. Colorado alone has collected over $1.6 billion in marijuana taxes since 2014, funding education, public health, and infrastructure projects. Washington state has generated over $3 billion. While projections may have been overoptimistic in some jurisdictions, this hardly constitutes a failure – it simply indicates a need for more realistic forecasting and better-designed tax structures.
Health Risks:
Cannabis, like any substance, carries certain risks. However, comparative risk assessments consistently show it’s less harmful than legal substances like alcohol and tobacco. Dr. David Nutt’s famous study published in The Lancet ranked alcohol as far more harmful to users and society than cannabis. To focus on potential cannabis risks while ignoring the well-documented devastation of legal substances reveals a problematic double standard.
Usage Patterns:
Youth cannabis use has actually declined or remained stable in many states following legalization, contradicting prohibitionist predictions. Meanwhile, increased use among adults reflects exactly what legalization was designed to accomplish – providing adults with safe, legal access to a substance many find beneficial for relaxation, creativity, or medical symptoms. The decline in youth consumption likely stems partly from reduced novelty and rebellion appeal once cannabis becomes a regulated product rather than a forbidden fruit.
To fully realize the promises of cannabis legalization, we need a more comprehensive approach that addresses the legitimate concerns while removing the artificial constraints that have hampered success.
First and foremost, federal legalization is essential. The current federal prohibition creates unnecessary complications for banking, research, interstate commerce, and taxation. It forces businesses to operate on a cash basis, creating security risks and inefficiencies. It prevents the development of national brands and economies of scale that could drive down consumer costs. And it maintains the Schedule I classification that hampers medical research and perpetuates stigma.
Second, home cultivation rights must be protected. Allowing adults to grow limited amounts of cannabis for personal use provides a safety valve against monopolistic market structures and excessive pricing. It empowers consumers, reduces black market incentives, and recognizes that cannabis is, fundamentally, a plant that people have grown for thousands of years. States that have embraced home grow rights like Michigan and Colorado have seen thriving legal markets alongside personal cultivation.
Third, we need sensible regulatory structures that protect public health without imposing unnecessary burdens. This includes reasonable testing requirements, clear labeling standards, and age restrictions. However, excessive regulations that serve only to limit market participation or drive up costs without clear public health benefits should be eliminated. The current system in many states has created oligopolistic markets where licenses cost millions, shutting out small businesses and social equity applicants.
Fourth, tax policies need recalibration. Excessive taxation, especially when layered across cultivation, processing, and retail levels, drives up consumer prices and fuels black markets. A simple, moderate tax based on potency or sale price would generate revenue while allowing legal markets to compete with illicit operations.
Finally, we need honest education about both the benefits and risks of cannabis. Fear-mongering and exaggeration undermine credibility, while dismissing legitimate concerns is equally problematic. The vast majority of consumers—likely over 95%—will never experience serious adverse effects. However, those with predispositions to certain mental health conditions, particularly adolescents whose brains are still developing, face higher risks that should be clearly communicated.
When we take a clear-eyed look at cannabis legalization’s mixed results, the solution becomes evident: we don’t need less legalization—we need more complete, thoughtful implementation. The problems cited by critics largely stem not from legalization itself, but from the compromised, piecemeal approaches that have characterized policy reform thus far.
Federal legalization with home cultivation rights would strike a devastating blow to illegal markets by allowing interstate commerce, normalizing banking relationships, and recognizing the fundamental right of adults to grow a plant for personal use. The black market doesn’t thrive because legalization failed; it thrives because our current approach is incomplete and inconsistent.
Overtaxing and overregulating legitimate cannabis businesses while maintaining federal prohibition creates the worst of all worlds—high consumer prices, limited access, and continued incentives for illicit operators. We can’t expect the black market to disappear when we’ve designed systems that actively advantage it.
The National Review article gets one thing right—we should indeed rethink marijuana legalization. But instead of retreat, we need to advance toward more coherent, evidence-based policies that truly put “We the People” at the center. Give Americans the freedom to grow their own cannabis, purchase from a diverse marketplace of businesses both small and large, and make personal health decisions without government interference.
Do that, and watch the promises of legalization—reduced black markets, significant tax revenue, controlled access for adults, and diminished criminal influence—finally come to fruition. It’s time to complete the journey we’ve started, not turn back halfway.
TRUMP 2.0 ON LEGAL WEED? READ ON…
WHAT TRUMP’S CANNABIS POLICIES MEAN FOR AMERICA AND THE WORLD!


In a move that has reignited debates about federal drug policy, former President Donald Trump has appointed Terrance Cole as the new head of the Drug Enforcement Administration (DEA). Cole, a veteran DEA official with over two decades of experience, is known for his staunch opposition to marijuana legalization. His appointment signals a return to the Reagan-era “Just Say No” approach to drug enforcement, with Cole publicly linking cannabis use to an increased risk of suicide and schizophrenia, particularly among young users.
The announcement has drawn sharp reactions from both sides of the political aisle, with advocates for cannabis reform expressing concern that Cole’s leadership could roll back progress made in recent years. Meanwhile, proponents of stricter drug enforcement have hailed the appointment as a necessary step to combat what they see as the growing normalization of marijuana in American society.
This article delves into Terrance Cole’s background, his controversial views on cannabis, and what his appointment could mean for the future of marijuana policy in the United States.
A Return to Hardline Drug Policies?
Terrance Cole’s appointment comes at a pivotal time for cannabis policy in the United States. Over the past decade, there has been a seismic shift in public attitudes toward marijuana. As of 2025, 23 states have legalized recreational cannabis use, and 38 states allow medical marijuana. Public opinion polls consistently show that a majority of Americans support federal legalization. Despite this momentum, marijuana remains classified as a Schedule I drug under the Controlled Substances Act—a category reserved for substances with a high potential for abuse and no accepted medical use.
Cole’s nomination appears to signal a departure from the more reform-oriented approach taken by previous administrations. During President Joe Biden’s tenure, there were significant discussions about rescheduling marijuana to a lower classification or even decriminalizing it at the federal level. However, Trump’s decision to appoint Cole suggests that his administration is doubling down on traditional drug enforcement strategies.
In his first public statement following his nomination, Cole said:
”We cannot afford to ignore the science. Marijuana is not the harmless substance that many claim it to be. It poses serious risks to mental health and public safety.”
This rhetoric echoes the anti-drug messaging of the 1980s, when First Lady Nancy Reagan spearheaded the “Just Say No” campaign as part of the broader War on Drugs. Critics argue that such policies disproportionately targeted minority communities and contributed to mass incarceration without effectively addressing substance abuse issues.
Who is Terrance Cole?
Terrance Cole is no stranger to the DEA or its mission. Over his 22-year career with the agency, he rose through the ranks, earning a reputation as a tough-on-crime enforcer. Before his nomination as DEA Administrator, Cole served as Special Agent in Charge of the agency’s Washington Field Division, where he oversaw high-profile operations targeting drug trafficking organizations.
Cole has long been an outspoken critic of marijuana legalization efforts. In 2021, he testified before Congress against proposals to decriminalize cannabis at the federal level. During his testimony, he cited studies suggesting that heavy marijuana use among adolescents could lead to long-term cognitive impairment and an increased likelihood of developing psychosis or schizophrenia.
”The data is clear,” Cole said during his testimony. ”Marijuana today is far more potent than it was 30 years ago. We are not dealing with Woodstock weed anymore; we are dealing with a substance that can have devastating effects on young minds.”
Cole has also linked cannabis use to rising suicide rates among teenagers and young adults. While some studies have explored potential correlations between heavy cannabis use and mental health issues, critics argue that such claims oversimplify complex issues and ignore other contributing factors like socioeconomic conditions and access to mental health care.
The Science Behind Cole’s Claims
Cole’s assertions about marijuana’s risks are not without precedent but remain highly contested within the scientific community. Some research has suggested a potential link between heavy cannabis use and mental health disorders like schizophrenia in individuals predisposed to such conditions. For example:
A 2019 study published in The Lancet Psychiatry found that daily use of high-potency cannabis was associated with an increased risk of psychotic disorders.
Other studies have suggested that early and frequent cannabis use may exacerbate symptoms in individuals already vulnerable to mental health issues.
However, many experts caution against drawing causal conclusions from these findings. Dr. Susan Weiss, director of the ”ivision of Extramural Research at the National Institute on Drug Abuse (NIDA), has stated:
”While there is evidence of an association between cannabis use and certain mental health outcomes, it is important to consider other variables that may contribute to these risks.”
Moreover, proponents of legalization argue that regulating marijuana can mitigate some of these risks by ensuring product safety and providing education about responsible use.
Implications for Federal Marijuana Policy
Cole’s appointment could have far-reaching consequences for federal marijuana policy. As head of the DEA, he will play a key role in determining how federal law enforcement approaches cannabis-related offenses. This includes decisions about whether to prioritize crackdowns on state-legal cannabis businesses or focus resources on other drug enforcement efforts.
One immediate concern among advocates is how Cole’s leadership might impact efforts to reschedule or deschedule marijuana under federal law. In October 2022, President Biden directed federal agencies to review marijuana’s classification as a Schedule I drug—a move widely seen as a step toward reform. However, with Cole at the helm of the DEA, such efforts could face significant resistance.
Kevin Sabet, president of Smart Approaches to Marijuana (SAM), praised Cole’s appointment as a victory for public health:
”Terrance Cole understands that we cannot sacrifice our youth’s well-being on the altar of Big Marijuana profits.”
On the other hand, organizations like NORML (National Organization for the Reform of Marijuana Laws) have expressed alarm over what they see as a regressive turn in federal policy. In a statement following Cole’s nomination, NORML Executive Director Erik Altieri said:
”This appointment represents an outdated approach to drug policy that ignores decades of progress and overwhelming public support for legalization.”
State vs. Federal Tensions
Cole’s hardline stance could exacerbate tensions between state governments that have legalized marijuana and federal authorities tasked with enforcing prohibition laws. While Congress passed legislation in 2023 protecting state-legal cannabis businesses from federal interference, these protections are not permanent and could be revisited under new leadership.
In states like Colorado and California—where legal cannabis industries generate billions in revenue annually—there is growing concern about how aggressive federal enforcement might disrupt local economies. Additionally, medical marijuana patients who rely on cannabis for conditions like chronic pain or epilepsy worry about potential restrictions on access.
The Broader Debate: Public Safety vs. Personal Freedom
At its core, Cole’s appointment reignites broader debates about how society should balance public safety concerns with individual freedoms when it comes to drug use. Supporters of stricter enforcement argue that normalizing marijuana sends mixed messages about its risks—particularly to young people—and undermines efforts to address substance abuse more broadly.
Opponents counter that criminalizing cannabis does more harm than good by perpetuating systemic inequalities and diverting resources away from addressing more pressing public health crises like opioid addiction.
Dr. Ethan Russo, a neurologist and prominent cannabis researcher, argues:
”We need policies grounded in science rather than fear-mongering rhetoric. Demonizing cannabis ignores its potential benefits while failing to address legitimate concerns about misuse.”
Conclusion
Terrance Cole’s appointment as DEA Administrator marks a significant shift in federal drug policy under former President Donald Trump’s administration. With his “Just Say No”-style rhetoric and firm opposition to marijuana legalization, Cole represents a return to more traditional approaches to drug enforcement—ones that many hoped were relics of the past.
As debates over cannabis reform continue to unfold at both state and federal levels, one thing is clear: Terrance Cole’s leadership will be closely watched by advocates on all sides of this contentious issue. Whether his tenure will lead to meaningful progress or further polarization remains an open question—but its impact on America’s evolving relationship with marijuana is likely to be profound.
THE DEA ON HEMP AND MARIJUANA, READ ON…

Save 30% all month long at The Dispensary Fulton

Ohioans activate to defend weed legalization from lawmakers

It All Turned A Bit Bogan At Aussie Medical Cannabis Symposium

Building cannabis brands that reach across markets

ILGM’s Home Grow Tour 2025

Karma Koala Podcast 238: Daniel Shortt Launches New Firm With Partner Perry Salzhauer In Pacific NW
Trump invites former cannabis prisoner to speech, but doesn’t mention cannabis (Newsletter: February 5, 2025)

How Cannabis Can Help You During Lent

Buddha Chief raises vibrations at new Housing Works dispensary in NoMad

3 best THCA vape carts of 2025 by Leafly

Distressed Cannabis Business Takeaways – Canna Law Blog™

United States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)

What you Need to Know

Drug Testing for Marijuana – The Joint Blog

NCIA Write About Their Equity Scholarship Program

It has been a wild news week – here’s how CBD and weed can help you relax

Cannabis, alcohol firm SNDL loses CA$372.4 million in 2022

A new April 20 cannabis contest includes a $40,000 purse

Your Go-To Source for Cannabis Logos and Designs

UArizona launches online cannabis compliance online course
-
 Cannabis News2 years ago
Cannabis News2 years agoDistressed Cannabis Business Takeaways – Canna Law Blog™
-
 One-Hit Wonders2 years ago
One-Hit Wonders2 years agoUnited States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)
-
 Cannabis 1012 years ago
Cannabis 1012 years agoWhat you Need to Know
-
 drug testing1 year ago
drug testing1 year agoDrug Testing for Marijuana – The Joint Blog
-
 Education2 years ago
Education2 years agoNCIA Write About Their Equity Scholarship Program
-
 Cannabis2 years ago
Cannabis2 years agoIt has been a wild news week – here’s how CBD and weed can help you relax
-
 Marijuana Business Daily2 years ago
Marijuana Business Daily2 years agoCannabis, alcohol firm SNDL loses CA$372.4 million in 2022
-
 California2 years ago
California2 years agoA new April 20 cannabis contest includes a $40,000 purse