

All about Cannabis
Raphael Mechoulam, RIP – Cannabis | Weed | Marijuana
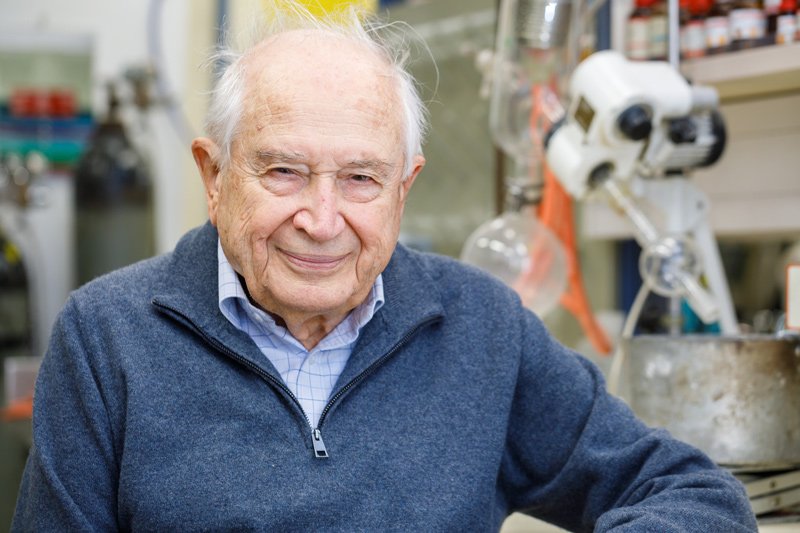
Raphael Mechoulam, the Israeli chemist who first isolated THC, died in his home. He was 92 years old.
The American Friends of the Hebrew University confirmed his death. Mechoulam had been a professor at the university since 1966.
Who Was Raphael Mechoulam?

Raphael Mechoulam was an Israeli organic chemist and professor of Medicinal Chemistry at the Hebrew University of Jerusalem. Cannabis research and Mechoulam are essentially synonyms.
This, of course, is likely due to his discovery and isolation of delta-9-tetrahydrocannabinol (THC), the primary psychoactive component of cannabis.
In the 1960s, Mechoulam and his research team were the first to identify and synthesize THC.
This not only illuminated the chemical structure and pharmacology of cannabis but eventually led to the discovery of the endocannabinoid system.
Medical cannabis wouldn’t be a thing without Mechoulam’s work. His work earned him the title “the father of cannabis research.”
Throughout his career, Mechoulam received numerous awards and honours for his contributions to the field of cannabis research, including the Rothschild Prize in Chemical Sciences and Physical Sciences, the Israel Prize in Exact Sciences, and the Lifetime Achievement Award from the International Cannabinoid Research Society.
Why Did He Study Cannabis?

Raphael Mechoulam’s interest in cannabis began in the 1960s when a cultural shift embraced the plant. But Mechoulam was more interested in science than culture.
“Morphine had been isolated from opium in the 19th century, early 19th century,” Mechoulam said in a 2014 interview. “Cocaine had been isolated from coca leaves mid-19th century. And here we were, mid-20th century, and yet the chemistry of cannabis was not known. So it looked like an interesting project.”
His team isolated THC and its effects on the brain and body. They also isolated other cannabinoids and their effects, including cannabidiol or CBD.
“I was surprised to note that an active compound had apparently never been isolated in pure form,” Mechoulam said. “And that its structure was only partially known. Even the structure of a major crystalline component, cannabidiol (CBD), which had been isolated more than two decades previously, was not fully elucidated.”
And while known as the father or grandfather of cannabis research, Mechoulam also researched the pharmacology of the khat plant, which many people in East Africa and the Middle East often use as a stimulant.
In the West, manufacturers often synthesize it into cathinones or “bath salts.”
“Most of the human and scientific knowledge about cannabis was accumulated thanks to Professor Mechoulam,” Asher Cohen, the president of the Hebrew University of Jerusalem, said in a statement. “He paved the way for groundbreaking studies and initiated scientific cooperation between researchers around the world. Mechoulam was a sharp-minded and charismatic pioneer.”
How Did Mechoulam Study Cannabis?

“When we started work many years ago, there was essentially no interest in cannabinoids,” Mechoulam said in a 2019 interview.
He applied for a grant from the National Institutes of Health (NIH) in the United States in the 1960s. They told him that Americans aren’t interested in “marijuana.” That it’s something only Mexicans use.
Eventually, the NIH reversed course and supported Mechoulam’s research. But this general attitude that cannabis was irrelevant in the 1960s shows that the NIH has always been out of touch.
The current head of its drug abuse sector is the great-granddaughter of Leon Trotsky. She has a clear bias toward the brain-disease model of addiction. Because of one person’s values, funding for research goes one way. It becomes like an ideology.
For Mechoulam living in Israel, where cannabis was also illegal, he made contacts within police departments for a steady supply. As he said in an interview, “I didn’t have a car at the time. I was on the bus carrying five kilos of hashish. People were just saying, ‘It’s kind of a strange smell.’ We tested that on a few volunteers, including ourselves.”
As Mechoulam wrote in the Annual Review, he and his team “extracted the hashish and, by repeated column chromatography, were able to isolate about 10 compounds — most of them unknown — and elucidate their structures.”
In 1980, he was in Brazil conducting CBD research on people with epilepsy. Within a few months, he and his team found that none of the people in the study reported seizures.
RIP
Of course, it’s always sad to hear about the passing of a great scientist and innovator like Mechoulam. We will remember his contributions to cannabinoid research for years to come.







What are the five cannabis stories you might have missed? Nowadays, it’s impossible to keep up with cannabis news stories across the world. Whether it’s banking reform and rescheduling in the United States, legalization in Europe or Thailand, or Canada’s experiment with corporate legalization.
Here are five cannabis stories you might have missed.
Five Cannabis Stories You Might Have Missed
Suing Over Cannabis Rescheduling

U.S. Attorney Matthew Zorn is suing the Biden Administration over cannabis rescheduling, particularly over the secrecy of it all. If you missed this cannabis story, here are the details.
Last month, the U.S. Health and Human Services Department (HHS) sent a letter to the Drug Enforcement Administration (DEA) suggesting they reschedule cannabis.
Currently, the U.S. government lists cannabis as a Schedule 1 drug, in the same category as heroin. The HHS letter suggests it should be a Schedule 3. Cannabis would still be a controlled substance but with fewer restrictions.
U.S. Attorney Matthew Zorn has filed an official complaint in the U.S. District Court. He says the letter “has become an item of public interest.” He has asked the court to force the Biden Administration to release “improperly held agency records.”
Zorn tried a Freedom of Information Act request but to no avail. HHS “has not produced the requested record” and “did not make a timely determination within 20 days,” the complaint alleges.
60% Higher Risk of Cardiovascular Problems Linked to “Cannabis Use Disorder”
Another day, another study finding an “association” between cannabis and something terrible. This time, it’s cardiovascular problems. You haven’t missed much if you missed this cannabis news story.
Here are some problems with the study:
Correlation is not Causation. Like most of these “cannabis is bad for you” studies, the researchers have merely made an association. Fortunately, this study explicitly states there is no causation. They simply found an association after controlling for variables.
Confounding Variables. While the study adjusts for some variables, it says it cannot account for tobacco smoking due to data limitations. This is obviously a significant limitation.
Smoking cigarettes is a far more significant risk factor for cardiovascular diseases than smoking cannabis.
Not being able to parse out this variable makes the study beyond useless. It’s literally disinformation. If you missed this cannabis news story, then you’re better off for it.
Five Cannabis Stories You Might Have Missed
Sampling Cannabis in British Columbia

You might have missed this cannabis story out of British Columbia, Canada.
After years of stigma and drug war propaganda, the British Columbia government is finally starting to loosen their cannabis rules and regulations.
Licensed producers can now provide samples for retailers. The Grow Up Conference and Expo was the first cannabis industry event to take advantage of the new rules.
Advocates say the new regulations will benefit the industry in several ways. Retailers will now be able to see the product they’re buying and sample it for their customers.
Unfortunately, retailers cannot provide samples to customers yet. But the industry is hopeful that it’s in the works. That’s undoubtedly a cannabis new story we wouldn’t want to miss.
Thailand To Reconsider Cannabis Decriminalization
You might have missed this vital cannabis news story: Thailand may re-criminalize cannabis.
Two years ago, Thailand became the first Asian country to decriminalize cannabis. But its government, led by Prime Minister Srettha Thavisin, has vowed to roll back cannabis legalization.
In an interview with Bloomberg Television in New York while attending the UN General Assembly, Srettah made clear that residents of the country will only be able to use cannabis for medical reasons.
“It’s just for medical reasons. We need to rewrite the law,” he said.
Current legislation has cannabis removed from a list of narcotics. Individuals are supposed to notify their local government if they want to cultivate plants at home. But so far, the government has not created any regulations regarding cultivation and sales.
This regulatory vacuum has created a “free-for-all” industry much like the “wild-west” of British Columbia before Justin Trudeau’s corporate cannabis takeover.
While some estimated Thailand’s cannabis market may be worth nearly $2 billion, the new government ensures that money will remain in the black market.
Five Cannabis Stories You Might Have Missed
SAFER Banking Almost a Reality

We covered this one, but you might have missed this important cannabis news story.
Less than a week after being re-introduced, the SAFER Banking Act found approval by the Senate Banking Committee on September 27. The committee voted 14-9 to advance the legislation to the Senate floor.
The text of the new amendment is not yet available publicly. But give it enough time, and U.S. Attorney Matthew Zorn may sue to get the details released.
But overall, thanks to this committee, the movement toward cannabis reform in the United States just got a shot in the arm.

What is Vivek Ramaswamy’s position on cannabis? “You don’t hear me talk about the war on drugs. I’m not a war on drugs person,” Ramaswamy said when he appeared at a Free State Project event in New Hampshire last June.
Vivek Ramaswamy is an American entrepreneur seeking the Republican nomination to run for President of the United States.
Ramaswamy told the crowd he was “probably the only person in the modern history” of the Republican Party to talk about decriminalizing drugs for people with PTSD and other mental health problems.
“Psychedelics,” he said specifically. “From ayahuasca to ketamine… That’s gotta be part of the solution.”
But what is Vivek Ramaswamy’s position on cannabis? He told Fox News:
We got to catch up with the times. It’s not a popular position in the Republican Party, but I’d just, again, I guess I’m going to speak the truth. Whether you vote for me or not is your choice. I think the time has come to decriminalize it.
Later, a spokesperson from his campaign said:
The current state-level ‘legalization‘ farce contributes to the culture of lawbreaking. It’s literally against the law. For us to pretend otherwise only undermines the rule of law in this country. For that reason, Vivek favors the federal legalization of marijuana.
What is Vivek Ramaswamy’s Position on Cannabis?

What is Vivek Ramaswamy’s Position on Cannabis? Decriminalization or legalization? Once upon a time, those meant the same thing. And indeed, in America, this may still ring true.
Vivek isn’t shy about wanting to rule by executive fiat. Suppose he’s the next U.S. President and unilaterally deschedules cannabis. Not a rescheduling, a complete descheduling.
As far as the federal government is concerned – cannabis is not its business.
Is that decriminalization or legalization? For operators in legal states, it certainly helps their tax situation. And why would the financial system fear a plant the government has delisted as a controlled substance?
Is that legalization or decriminalization? Or are those terms synonymous?
If a Ramaswamy Administration removed cannabis from the Controlled Substances Act entirely, there would be a few implications.
Implications of De-Scheduling Cannabis

Vivek Ramaswamy’s position on cannabis could empower state-level regulations. If the federal government takes a literal hands-off approach, you could argue that’s not legalization.
But is legalization ideal? Should Washington D.C. force states like Idaho to legalize? Suppose people in Idaho want to consume cannabis legally. There are 23 other states they can move to, including next-door neighbors.
Even if all 50 states legalized – isn’t it better to have local regulation of a competitive and complex modern industry? Think of the supply chain: cultivation, production, packaging, distribution, sales, marketing, and everything in between.
Do you want D.C. bureaucrats in charge of all that? Isn’t that how lobbyists capture the process and rig the rules against the little guys?
When The Feds Do Get Involved
Of course, some will argue Vivek Ramaswamy’s position on cannabis can’t be entirely hands-off. Somebody is going to have to regulate interstate commerce and international trade.
Imports and exports are federal jurisdiction and always have been. Of course, Vivek’s brand of governing may detest interstate regulation. A Ramaswamy Administration may create a free-for-all for all industries, not only cannabis.
One can hope.
And, of course, FDA bureaucrats will want to control aspects of cannabis, especially if it’s used in food products or marketed as a medical treatment. In a sense, descheduling and taking a hands-off approach empowers the existing bureaucracy.
But Vivek can use the stroke of the Presidential pen and tell the FDA to buzz off. Such is the state of the American “republic.”
Of course, if Vivek Ramaswamy becomes President, he won’t be able to decline the tax revenue. Who can, really? Except for maybe Ron Paul.
So, the federal government may tax cannabis. And so Vivek Ramaswamy’s position on cannabis matters a great deal.
But there’s something else. And it involves Vivek’s policy on the Federal Reserve Bank.
Vivek Ramaswamy’s Position on Cannabis & Money Could Change the World

Vivek Ramaswamy’s position on cannabis and money could change the world. And here’s how.
Experts must control money. That’s what the experts say. That’s why supply and demand don’t determine interest rates. You can’t trust free markets, they say. You need a central planning committee of experts.
But when the hell has that ever worked? This is not the 1920s, this is the 2020s. We have evidence of central planning, and the results are far worse than any of the theoretical excesses of free-market capitalism.
But suppose the experts are right about one thing. The price of money is too volatile to leave to a truly random process. That there should be a more market-based approach to price stability.
As in, leave it to the experts, but not the boardroom suits. Leave it to the people who are actually buying and selling in the market on a daily basis.
Like Vivek Ramaswamy’s position on cannabis, his proposal for the Federal Reserve is a breath of fresh air—a novel idea in an age of corporate-state shallowness.
What is a Government Gold Standard?

A country on a gold standard exchanges its currency for gold at a fixed rate, say, $35 an ounce. And vice versa. So, if the market price of gold goes beyond $35, people bring in their dollars to exchange for gold.
This process means the number of dollars in circulation decreases, so the value of the dollar increases. This continues until the market price of gold is back to $35.
If the market price drops below $35, the same process works in reverse. Historically common, it’s not without its flaws. Governments tinker with the mechanism like a curious 12-year-old who takes apart the television to see how it works (and ends up breaking it in the process).
A gold standard keeps the value of the money constant relative to the market price of gold. Economists have all kinds of critics and rebuttals as to why that wouldn’t work today in the “modern” economy.
To their credit, relying on gold as the sole commodity backing the government currency does run into problems. Especially when governments are always trying to cheat the system.
Vivek Ramaswamy’s position on cannabis stems from listening to the people and the real experts (i.e. not “public health”). He is responding with the correct answers. He has – more or less – done the same with the subject of the Federal Reserve and the money.
What is a Commodity Bundle Standard?

Vivek Ramaswamy should combine his positions on money and cannabis.
Vivek wants a commodity bundle standard to help solve the problem of using government currency. In this system, the market defines the U.S. Dollar as a collection of commodities. This collection or bundle is valued by what’s in it.
For example, suppose you had one million dollars. You take it to the bank and demand your bundle. It could consist of a few pounds of gold and silver, but it’d mostly be a claim on commodities (i.e. 100 pounds of grade A beef, 10 barrels of crude oil, 1,000 board feet of lumber).
Likewise, anyone who brings in a bundle (the claim on commodities) gets a million dollars. This keeps the bundle’s price at a million dollars and, thus, a stable purchasing power, assuming nobody is messing with the bundle.
Vivek Ramaswamy’s Position on Cannabis & Money Could Change the World
Vivek Ramaswamy could combine his positions on money and cannabis by including 1,000 pounds of industrial hemp biomass and 500 grams of premium-grade cannabis flower in the commodity bundle.
Regarding “changing the world,” you’ll have to refer to some of our past posts on the subject.
The main takeaway: eliminating the elite’s ability to create money out of thin air and charge interest on it can only be construed as a step in the right direction.
In fact, it’s the first step.

Regulating cannabis like fish? Excuse me, what? According to Leah Heise, the cannabis industry can learn much from commercial fishing.
An accomplished cannabis exec, Leah’s been the CAO of Ascend Wellness Holdings, the CEO of Women Grow, CXO of 4Front Ventures and President of Chesapeake Integrated Health Institute.
While at Ascend, Leah focused on growing the business from 73 employees to more than 1300 in less than 18 months, taking the company from $19M in revenue in 2019 to a $1.6B market cap in 2021.
Leah is also a medical cannabis patient, having discovered the herb after being hospitalized over 35 times for pancreatitis.
Leah Heise is a cannabis expert. Her expertise is unparalleled, unlike the so-called “experts” in the media who spew drug war propaganda.
So when she says the cannabis industry has much to learn from commercial fisheries, our ears perk up.
Regulating cannabis like fish? Say what?
Regulating Cannabis from Stigma

Having experience in the regulatory landscape, Leah knows what’s working and what’s doomed to fail. And unfortunately, most legal states have been regulating cannabis from a position of stigma.
“We do everything by piecemeal, by litigation. It’s very costly to the system and there’s just a better, more streamlined way to do it,” says Leah. “And I think that potentially regulating it similar to a commercial fishing industry may be the way to do it.”
Of course, Leah points out that there are other options, and this is just one of many ideas. But, she says, “These regulators need to understand the things they are regulating.”
“They’re doing it from a place of stigma and lack of education,” Leah says. “We have to turn back one hundred years of stigma and propaganda.”
Whether it’s racial stigma or false beliefs that cannabis will rot your brain, Leah emphasizes education. From scientific papers proving cannabis’ efficacy to patient stories to studies that associate legal cannabis with fewer cases of domestic abuse and alcoholism.
“The industry and the plant need a rebrand,” says Leah. “It’s not Cheech and Chong. It’s everyone; it’s diverse. Anybody could be using this, from your great-grandmother to your child, depending on what they have. It’s not going to make their brains die or reduce IQ.”
Regulators Need Education
Simply put, the public (and many regulators) are uneducated on cannabis. Drug warriors amplify its alleged harms while marginalizing its medical and therapeutic benefits.
But how would regulating cannabis like fish help? Leah admits that if the feds get involved, a strong regulatory body needs to be created.
“Or just let the states do it,” she says. “We don’t necessarily need another layer on top.”
But suppose the federal government does step in and institute national cannabis regulations. What can we learn from the commercial fishing industry?
Regulating Cannabis like Fish

What can the cannabis industry learn from commercial fishing? How does one regulate cannabis like fish?
“Fisheries is a highly regulated industry,” says Leah. “Because the government’s trying to balance the interests of the environmental groups with the interest of the commercial fishing industry.”
Yes, they are separate products, but both are natural and come from the Earth. Likewise, generations of people work in the industry, whether it’s multiple generations of fishermen (and women). Or the legacy farmers in the cannabis industry (especially in black and brown communities).
With the commercial fishing industry, there’s the problem of overfishing. “In an effort to save the planet, and the fisheries themselves, the federal government has stepped in,” says Leah.
And she sees opportunities for the cannabis industry and its regulators to learn from the commercial fishing industry.
Commercial fishing regulators don’t regulate from a place of stigma. “I haven’t seen a single state,” says Leah, referring to legal cannabis states, “where there’s not a massive lawsuit. And even with Schedule III, there’s going to be lawsuits.”
Learning from the Commercial Fishing Industry
Leah prefers a more comprehensive way of regulating cannabis, which borrows from the successes of the commercial fishing industry.
“They design things called fishery management plans,” she says. “Scientists in the government will come forward and say, ‘okay we’re starting to see Atlantic sea scallops start to collapse. We’re seeing a decline in the number of new pollock. And we need to come up with a fishery management plan to work this.’”
Leah says the commercial fishing industry has councils with different stakeholders, from environmental groups to commercial industries to recreational groups.
“They come together to regulate themselves,” says Leah. “It speeds up the process and really eliminates a lot of the issues in terms of getting sued, because stakeholders at least feel like they have a voice.”
“Nobody walks away happy,” Leah adds. “Which is kind of what happens with any real decent negotation, right? Everybody’s giving a little.”
Leah thinks having a board of stakeholders would prevent things like canopy caps or taxing inside the supply chain. Things that ultimately hurt the industry and only empower illicit markets.
The problem, says Leah, is that current cannabis regulators “aren’t holistically looking to see what the impacts are,” of the various regulations they’ve instituted.
Regulating Cannabis like Fish – Unintended Consequences?

Is there any state already doing this? What are the odds D.C. will create cannabis regulations that embody the principles of the commercial fishing industry?
One of the biggest problems, says Leah, is the lack of money on the enforcement side. From her regulator days, Leah recalls:
We were handed often times very dense regulations to enforce. But we weren’t given the money that we needed to be given to it, to hire the people, and train the people we needed to actually enforce those regulations.
The result is cannabis operators openly flaunting the rules because paying the fines is sometimes cheaper than observing the regulations.
There’s also debate on how heavy cannabis regulations should be. Should we regulate it like alcohol? Or should we consider cannabis a vegetable no more dangerous than a carrot?
“I think that the polarization that exists in this industry exists in the country,” says Leah, so there’s no easy answer.
Unintended Consequences

But one thing to watch out for is the unintended consequences of regulation. Leah recalls visiting Africa, particularly Botswana, about a year ago.
“The Gates Foundation had contributed billions of dollars worth of mosquito nets,” Leah recalls.
They thought that giving people mosquito nets would eliminate malaria. But what they didn’t understand is that [the Bostwanans] needed food. So what the people did was they used the nets to fish with. But the nets were covered with pesticides. It killed off all the fish. And you still have malaria, and you have no food, and it’s because there wasn’t really a holistic decision in that instance. [The Gates Foundation] wasn’t informed enough to answer what the real primary need was.
Unintended consequences are an unavoidable fact of life. In Canada, for example, the government legalized cannabis from a position of stigma and propaganda. The result is a thriving black market catering to consumer demands the legal market can’t fulfil.
With that in mind, we asked Leah how likely, on a scale of one to ten, would the United States legalize and regulate according to rational and holistic principles? Will authorities regulate cannabis like fish?
If ten is the ideal and one is stigma and propaganda, what’s the verdict?
“I think it’s going to be less than 5,” says Leah. And like the situation in Canada or the more restricted US legal states, the consequences of regulating from stigma suggest a robust illicit market.
“You can decide to go the legal route or you can decide to go the illegal route,” says Leah. “But you’re not going to make it go away.”

Pot prohibition costs Florida at least $200 million per year

Union’s initiative to organize Oregon marijuana workers nears ballot

Cannabis and Mental Health: Recent Research and Implications

Why You Shouldn’t Vote for Kamala Harris Just Because of Her Position on Cannabis- Banana in the Tailpipe, Again?

Your Trusted Amsterdam Seed Bank – Powered by Mother Nature, Breeding since 1996

Sam Hilliard’s clutch homer, Ezequiel Tovar’s walk-off send Rockies to win over Red Sox in 12 innings

Keeler: Trevor Story returned to Denver, but it was Rockies fan, transplant survivor who rocked Coors Field

As Trevor Story returns to Coors Field for first time since signing with Red Sox, injury-riddled shortstop remains confident he can regain old form

More RTD "slow zones" added as summer repairs move forward

Canadian wildfire smoke triggers poor air quality, health advisories in Colorado

Distressed Cannabis Business Takeaways – Canna Law Blog™

United States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)

What you Need to Know

Drug Testing for Marijuana – The Joint Blog

Cannabis, alcohol firm SNDL loses CA$372.4 million in 2022

NCIA Write About Their Equity Scholarship Program

It has been a wild news week – here’s how CBD and weed can help you relax

City Of Oakland Issues RFP For Employee Training Programs

A new April 20 cannabis contest includes a $40,000 purse

Your Go-To Source for Cannabis Logos and Designs
-
 Cannabis News1 year ago
Cannabis News1 year agoDistressed Cannabis Business Takeaways – Canna Law Blog™
-
 One-Hit Wonders1 year ago
One-Hit Wonders1 year agoUnited States: Alex Malyshev And Melinda Fellner Discuss The Intersection Of Tax And Cannabis In New Video Series – Part VI: Licensing (Video)
-
 Cannabis 1011 year ago
Cannabis 1011 year agoWhat you Need to Know
-
 drug testing7 months ago
drug testing7 months agoDrug Testing for Marijuana – The Joint Blog
-
 Marijuana Business Daily1 year ago
Marijuana Business Daily1 year agoCannabis, alcohol firm SNDL loses CA$372.4 million in 2022
-
 Education1 year ago
Education1 year agoNCIA Write About Their Equity Scholarship Program
-
 Cannabis1 year ago
Cannabis1 year agoIt has been a wild news week – here’s how CBD and weed can help you relax
-
 Education1 year ago
Education1 year agoCity Of Oakland Issues RFP For Employee Training Programs